Module 1: Introduction to Birth Doula Work — 8 Hours
Topics Covered:
Definition of a birth doula
The history and evolution of doula work
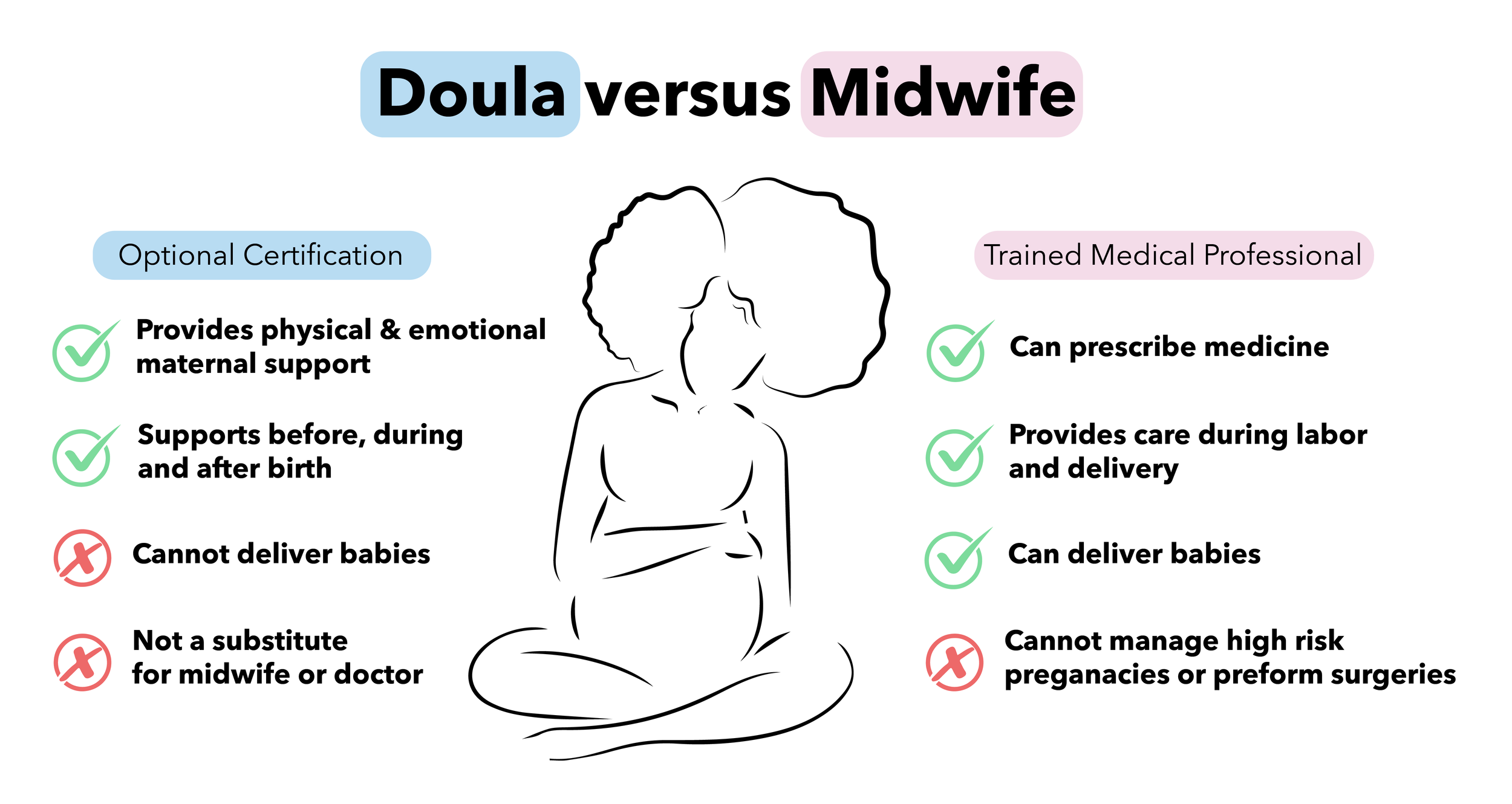
Distinguishing between a doula, midwife, and other birth professionals
IN THIS LESSON

Introduction
When families prepare for birth, it’s natural to have questions about who will be by their side and what roles each professional plays. While doctors and midwives provide essential medical care, doulas offer something different but equally important: continuous emotional, physical, and informational support. In this lesson, we’ll explore exactly what a birth doula is, trace the history and evolution of doula work, and clarify how doulas differ from midwives, nurses, and other professionals. By the end, you’ll understand how each role fits together to create a supportive birth team.

Unit 1 · Lesson 1
Definition of a Birth Doula
Who we are, what we do, and where our role begins and ends
Learning objectives
- Define what a birth doula is and describe the scope of their role across pregnancy, labor, and the early postpartum period.
- Explain the three pillars of doula support — emotional, informational, and physical — and identify examples of each.
- Distinguish clearly between the role of a birth doula and that of medical providers such as nurses, midwives, and physicians.
Where does the word "doula" even come from?
Before you can define what a doula does, it helps to understand where the word comes from — because the etymology itself tells you something important about the role.
The word doula comes from ancient Greek: δούλα, meaning "woman servant" or "woman who serves." It was first used in a modern professional sense by medical anthropologist Dana Raphael in her 1973 dissertation-turned-book The Tender Gift: Breastfeeding, where she used the term to describe a supportive female companion who helps a new mother through the postpartum period — particularly with breastfeeding. Raphael was the first scholar to apply this word to the childbirth support role.
The term gained traction as a birth-specific descriptor in the 1980s when physician-researchers Marshall Klaus and John Kennell began their landmark clinical trials on the effects of continuous support during labor. Their work, along with colleagues Phyllis Klaus, Penny Simkin, and Annie Kennedy, led to the formal professionalization of the doula role — and launched a body of research that continues to grow today.
1973
Dana Raphael first uses "doula" in print (Embryo Project Encyclopedia, 2018)
1980s
Klaus & Kennell publish clinical trial findings on continuous labor support
1992
First professional doula training organization founded in North America
2017–present
Cochrane meta-analysis & policy integration globally; Medicaid coverage expanding
Why the etymology matters
Think of "service" not in a subordinate sense, but in the way a skilled guide serves a traveler. A doula serves the birthing person's experience, preferences, and sense of safety — not the institution, not the clock, and not anyone else's agenda. The word itself is a compass for the role.
How the research defines the role
Rather than relying on any single organization's definition, the peer-reviewed literature has converged on a remarkably consistent description of the birth doula. Across dozens of studies, clinical reviews, and meta-analyses, researchers define a birth doula in nearly identical terms:
"A doula is a trained maternal support professional who offers emotional, informational and/or psycho-social care during pregnancy, childbirth and/or the postpartum periods. Doulas do not replace but complement the role of clinicians (physicians, midwives and nurses)."— Patient-Centered Outcomes Research Institute (PCORI) systematic review, 2023
"Doulas are trained, non-medical providers who provide emotional, informational, and physical support during pregnancy, labor, and the postpartum period."— Kozhimannil et al., qualitative study on community doula implementation, PMC, 2024
"Doulas are non-medical childbirth companions [who] provide emotional, informational, physical, and advocacy support to people during pregnancy, birth, and postpartum."— Springer Nature: Maternal and Child Health Journal, 2025
Notice what is consistent across all three: non-medical, trained, continuous presence, three core types of support (emotional, physical, informational), and a complementary — not competing — relationship with clinical providers. These are not organizational talking points. They are the operational definition the scientific literature has reached through decades of research.
Let's unpack each of these key terms.
Trained. A doula is not a well-meaning friend who happens to be present. Training equips doulas with knowledge of labor physiology, comfort techniques, communication skills, and professional ethics. The depth of that training varies across certifying bodies, but the research consistently identifies "trained" as a critical modifier — studies that compare trained doulas to untrained support persons show meaningfully stronger outcomes with the trained role (Bohren et al., 2017).
Non-medical. This is not a limitation — it is a defining feature. The doula's power comes precisely from occupying a different space than clinical providers. Research notes that because doulas hold no clinical responsibilities, they are free to remain entirely focused on the birthing person's emotional and physical experience, without shift rotations, competing patients, or documentation duties (Hodnett et al., 2013).
Continuous. This is one of the most clinically significant words in the literature. A doula stays from the onset of active labor through birth and into the immediate postpartum period without breaks. Research on why continuity matters is addressed in depth below.
The three pillars of doula support
All doula support falls within three interconnected domains, consistently identified across the peer-reviewed literature (Hodnett et al., 2013; Bohren et al., 2017; Sobczak et al., 2023; Ramey-Collier et al., 2023):
❤ Emotional
Continuous presence, reassurance, encouragement, holding space for fear and joy, supporting partners, building trust before and during labor.
🤲 Physical
Comfort measures: massage, counter-pressure on the sacrum, positioning guidance, heat/cold application, movement facilitation, hydration reminders.
📚 Informational
Explaining what's happening during labor, helping clients formulate questions for their providers, reviewing birth preferences, and translating medical language into accessible terms.
A fourth element — advocacy — appears in some research definitions (Hodnett et al., 2013; Springer Nature, 2025) and is addressed separately below, because it is the most frequently misunderstood component of the role.
Seeing all three pillars at once
Imagine your client is 7 cm dilated and beginning to doubt herself, saying "I can't do this anymore." Emotional support: move close, make eye contact, say "You are doing it — you're in transition and that means you're almost there." Physical support: apply firm counter-pressure to her sacrum during the next contraction. Informational support: explain that transition — the hardest phase — is also the shortest. All three happen in the span of three minutes. The research literature describes this layered approach as the defining quality of trained doula care (Bohren et al., 2017).
The scope of the doula relationship: before, during, and after
Prenatal (before birth)
Most doulas meet with clients two to three times during pregnancy. These meetings serve several purposes: building rapport, learning the client's values and concerns, reviewing birth preferences, educating about the stages of labor, and orienting the support partner to their role. Morton and Clift (2014) describe this prenatal relationship as foundational — the trust established before labor directly shapes how effective the doula can be once labor begins.
Why prenatal visits matter so much
Consider two doulas showing up at the same birth center at 3 a.m. One has met the laboring person twice, knows she is frightened of losing control, that sacral pressure is her greatest discomfort, and that her partner tends to go quiet when anxious. The other is meeting the family for the first time. Same skills — completely different effectiveness. Prenatal relationship-building is not administrative. It is the clinical work of the doula role.
Intrapartum (during labor and birth)
This is the core of birth doula work. The doula provides continuous presence from the time they are called through birth and into immediate postpartum recovery. Research by Gilliland (2010) details the specific emotional support strategies doulas use during this period — including reflective listening, encouragement, mirroring, and "protecting an atmosphere of quiet focus." Physical support techniques are likewise specific: positioning for pain relief or labor progress, use of breath, sacral counter-pressure, and application of cold and heat (Gilliland, as cited in Bohren & Tunçalp, 2018).
Postpartum (shortly after birth)
Most birth doulas remain for one to two hours after delivery to support initial bonding and early feeding. Many follow up within the first week to debrief the birth experience and provide referrals. Research notes that the emotional processing of birth — regardless of how it unfolded — is itself a significant need that doulas are uniquely positioned to address (Sobczak et al., 2023). This is distinct from postpartum doula work, which is a separate specialization focused on the weeks following birth.
What a doula is not: knowing the boundaries
The research literature is clear and consistent on this point: a doula does not perform clinical or medical tasks, does not diagnose, does not prescribe, and does not make medical decisions on behalf of the client (Hodnett et al., 2013; PCORI, 2023; Ramey-Collier et al., 2023). This is not a regulatory technicality — it is the structural condition that makes the doula role possible and effective. The doula's non-clinical status is precisely what allows them to be present continuously and to remain entirely focused on the birthing person's experience.
When clinical training and doula work overlap
Research and scope-of-practice literature consistently note that professionals who hold clinical training (nursing, midwifery, etc.) cannot apply those clinical skills while acting in a doula role. The role is defined by what services are being provided — not the professional's background alone. This protects clients, the care team, and the doula from role confusion that research has identified as a source of interprofessional conflict (Bohren & Tunçalp, 2018).
The clearest way to understand this is through direct comparison:
| Domain | Birth Doula | Nurse (L&D) | Midwife / OB |
|---|---|---|---|
| Clinical assessments | No — does not check dilation, assess fetal heart tones, or conduct exams | Yes — full monitoring and assessment | Yes — full clinical scope |
| Medications / IV | No — cannot administer or recommend medications | Yes — administers under orders | Yes — can prescribe and administer |
| Continuous presence | Yes — stays with client throughout entire labor | Limited — shared between patients, monitoring duties, charting | Limited — arrives for active/late labor and birth |
| Emotional support | Core role — primary focus | Important but secondary to clinical duties | Valued but not the primary role |
| Speaks for client | No — facilitates communication, amplifies client's voice; never replaces it | Advocates within clinical role | Advocates within clinical role |
| Decision-making | No — helps client access information; client makes all decisions | Informs and documents decisions | Makes clinical recommendations |
| Relationship start | Prenatal — weeks or months before birth | Beginning of assigned shift | Established in prenatal care, or on-call basis |
Research has documented that nurses in labor and delivery settings spend only 6–10% of their time engaged in labor support activities, primarily due to documentation demands, staffing constraints, and competing patient responsibilities — while birthing people expect 53% of nursing time to be focused on support (Tumblin & Simkin, 2001; Gagnon et al., 1997, as cited in Ballen & Fulcher, 2006). This gap is not a criticism of nursing — it is the structural reality that explains why continuous doula support is a distinct and necessary role.
Scenario to consider
Your client's nurse has just said she needs to remain in bed for continuous monitoring. Your client is upset and asks you: "Can I just ignore that? You said I could move around."
A doula does not contradict the nurse, make the clinical call, or project their own birth philosophy onto the situation. Instead: "That's a really important question — let's ask the nurse together why continuous monitoring is needed right now, and whether there's any flexibility in how you can be positioned. You have every right to understand what's happening and to ask questions." You are the bridge, not the decision-maker. This is precisely how the research describes the advocacy function (Bohren & Tunçalp, 2018; Hodnett et al., 2013).
Advocacy: the most misunderstood part of the role
The concept of "advocacy" in doula work has attracted significant attention — and some criticism — in the research literature. A 2018 paper in Health Expectations (Jenkinson et al.) specifically examined ethical tensions in how advocacy is defined and practiced, noting that some training frameworks promote an "active advocacy" model that can cross into making decisions on behalf of clients or challenging providers in ways that create conflict.
The authors propose grounding the doula's role in the framework of relational autonomy — a bioethical concept that recognizes that people make choices in a social context, not in isolation. From this perspective, a doula supports autonomy not by speaking for the client, but by helping the client feel emotionally secure enough, informed enough, and supported enough to make and communicate their own choices.
"Grounding the definition of the doula's role in relational autonomy gives coherence and guidance to the work doulas do and has the potential to resolve the kinds of conflicts and misunderstandings that have been reported."— Jenkinson, Josey & Flemmer, Health Expectations, 2018 (PMC5810740)
In practice: advocacy means helping clients clarify and voice their own wishes, encouraging them to ask questions, and supporting them to engage with their care team from an informed and grounded place. The goal is always to amplify the client's voice — not substitute for it.
The interpreter analogy
Think of your role as an interpreter in a high-stakes conversation. A skilled interpreter does not edit the message, add their own opinions, or argue on one party's behalf. They ensure clarity flows in both directions. That is your role in the birth room. The words belong to your client. Your job is to help them find and use those words even under enormous physical and emotional pressure.
What the evidence says: why this role matters
Understanding the definition of a birth doula is enriched considerably by understanding the research that established why this role was formalized. This is not a wellness trend — it is one of the most robustly studied non-pharmacological interventions in perinatal care.
Bohren et al. (2017) — Cochrane systematic review
Continuous Support for Women During Childbirth synthesized 27 randomized controlled trials involving nearly 16,000 women across 17 countries. Women with continuous labor support were more likely to have spontaneous vaginal births and shorter labors, and were less likely to need pain medication, have instrumental or cesarean births, or have newborns with low five-minute Apgar scores. The review found no evidence of harm in any outcome studied. Effects were greatest when support was provided by a trained person in a dedicated doula role — not hospital staff and not a social network member. (Bohren, Hofmeyr, Sakala, Fukuzawa & Cuthbert, Cochrane Database Syst Rev. 2017;7:CD003766.)
Collins et al. (2024) — American Journal of Public Health
A study of 722 matched pairs of Medicaid enrollees found that people with doula support had a 47% lower risk of cesarean delivery, a 29% lower risk of preterm birth, and were 46% more likely to attend a postpartum check-up. The researchers concluded that doula care is associated with meaningfully improved health outcomes in a Medicaid population. (Am J Public Health. 2024;114(11):1275–1285.)
Ramey-Collier et al. (2023) — Obstetrical & Gynecological Survey
A PubMed literature review of 34 original and review articles found that doula support is associated with increased vaginal delivery, decreased preterm birth and low birth weight, and is "a promising strategy to reduce healthcare inequities" — with evidence that effects are particularly strong for Black patients. (Obstet Gynecol Surv. 2023;78(2):124–127.)
Why presence itself is the intervention
Imagine running a marathon with a pace coach who runs every single mile beside you — versus one who checks in at miles 5, 13, and 26. Both care about your finish. Only one is actually there when the wall hits at mile 18. That's the difference between a doula and intermittent support. Labor, like a marathon, does not pause courteously while help is elsewhere. The Cochrane meta-analysis confirms this: it is the continuity of trained doula support — not any single technique — that accounts for the magnitude of the outcomes observed.
A quick summary: what doulas do and don't do
- Provide continuous, unbroken presence from active labor through immediate postpartum
- Offer physical comfort measures — massage, positioning, heat/cold, movement guidance
- Give emotional support, reassurance, and encouragement throughout labor
- Share evidence-based, non-medical information with clients and their partners
- Help clients formulate questions and communicate their preferences to the care team
- Support the birth partner in feeling confident and useful
- Facilitate — rather than lead — communication with clinical providers
- Perform clinical exams or assessments of any kind
- Administer or recommend medications
- Make medical decisions or provide medical advice
- Speak instead of the client or override client decisions
- Replace the role of the midwife, nurse, or physician
- Perform clinical tasks even if trained to do so in another professional role
🧠 Check your understanding
1
In your own words, explain the difference between advocacy and decision-making in a doula's role. Using Jenkinson et al. (2018), how does the concept of relational autonomy help clarify this distinction?
2
A client in labor asks you, "Do you think I should get the epidural?" Walk through how you would respond, drawing on all three pillars of support and the principle of informed, autonomous decision-making.
3
A labor and delivery nurse tells a client's family, "The doula is basically just here to cheer her on." How would you accurately and professionally explain the doula's role — and what research might you point to?
4
The Bohren et al. (2017) Cochrane review found the greatest outcomes when support was provided by someone in a "doula role" — not hospital staff, not a family member. Why do you think that distinction matters? What structural features of the doula role explain this finding?
Peer-reviewed references
- Bohren, M. A., Hofmeyr, G. J., Sakala, C., Fukuzawa, R. K., & Cuthbert, A. (2017). Continuous support for women during childbirth. Cochrane Database of Systematic Reviews, 7, CD003766. https://doi.org/10.1002/14651858.CD003766.pub6
- Collins, C., Bai, R., Brown, P., Bronson, C. L., & Farmer, C. (2024). Role of doulas in improving maternal health and health equity among Medicaid enrollees, 2014–2023. American Journal of Public Health, 114(11), 1275–1285. https://doi.org/10.2105/AJPH.2024.307805
- Jenkinson, B., Josey, N., & Flemmer, M. C. (2018). Defining the doula's role: Fostering relational autonomy. Health Expectations, 21(1), 130–139. https://doi.org/10.1111/hex.12604 [PMC5810740]
- Ramey-Collier, K., Jackson, M., Malloy, A., McMillan, C., Scraders-Pyatt, A., & Wheeler, S. M. (2023). Doula care: A review of outcomes and impact on birth experience. Obstetrical & Gynecological Survey, 78(2), 124–127. https://doi.org/10.1097/OGX.0000000000001103
- Sobczak, A., Taylor, L., Solomon, S., Ho, J., Kemper, S., Phillips, B., … & Jacobs, R. J. (2023). The effect of doulas on maternal and birth outcomes: A scoping review. Cureus, 15(5), e39451. https://doi.org/10.7759/cureus.39451 [PMC10292163]
- Hodnett, E. D., Gates, S., Hofmeyr, G. J., & Sakala, C. (2013). Continuous support for women during childbirth. Cochrane Database of Systematic Reviews, 7, CD003766. https://doi.org/10.1002/14651858.CD003766.pub5
- Patient-Centered Outcomes Research Institute. (2023). Impact of doula support during pregnancy, childbirth and beyond: A systematic review. https://www.pcori.org/research-results/2023/impact-doula-support-during-pregnancy-childbirth-and-beyond-systematic-review
- Al-Adeli, N., et al. (2025). Role of doulas across the pregnancy care continuum on maternal and child health: A scoping review. npj Women's Health. https://doi.org/10.1038/s44294-025-00109-4
- Raphael, D. (1973). The tender gift: Breastfeeding. Prentice-Hall. [First scholarly use of the term "doula"]
- Morton, C. H., & Clift, E. (2014). Birth ambassadors: Doulas and the re-emergence of woman-supported birth in America. Praeclarus Press.
A Day in the Life of a Doula at NewYork-Presbyterian Brooklyn Methodist Hospital
A group of women in NYC is fighting to make doulas accessible to everyone
Featured Study

Gruber, K. J., Cupito, S. H., & Dobson, C. F. (2013). Impact of Doulas on Healthy Birth Outcomes.
Gruber, K. J., Cupito, S. H., & Dobson, C. F. (2013). Impact of doulas on healthy birth outcomes. PMC3647727. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3647727/
Summary:
This study compared pregnant people who had a certified doula with those who did not, while all participants were in a prenatal education program. Those with doulas were four times less likely to have a low-birth-weight baby and twice as likely to avoid a birth complication. They were also significantly more likely to initiate breastfeeding. The doula helped by providing continuous presence, physical comfort, and emotional encouragement throughout pregnancy and birth. Doulas assisted in guiding communication between the birthing person and clinical caregivers. The research suggests this one-on-one support contributed to better experiences and outcomes. Although counseling and case support were also provided to all participants, the additional doula presence correlated with measurable positive differences.
What It Means to Birth Doulas:
For doulas, this research highlights the value of continuous support—an element central to doula work. It shows how non-medical assistance (comfort, presence, information) relates to key birth outcomes like birth weight and breastfeeding. The study supports the idea that doulas help build confidence and agency in birthing people. It also underscores the role doulas play before labor, not just during labor. This helps doulas advocate for earlier engagement in prenatal care. For doula programs, the findings justify emphasizing holistic support strategies. Clinically, it provides evidence that doula care can complement medical care, especially for socially disadvantaged clients.
Translating for Doula Clients:
When talking with clients, emphasize how continuous support makes a meaningful difference:“Research shows that having a doula is linked with fewer birth complications and a greater chance of successful breastfeeding. I’ll be with you through pregnancy, labor, and early postpartum so you feel empowered and understood.”
You can also tie outcomes to comfort and confidence:“Studies find people with doulas build better communication with their care team and feel more in control of their birth.”
This helps normalize doula support as evidence-based. Reinforce that your role is supportive, complementary, and focused on their goals. Invite questions about preferences in care to build trust.

Unit 1 · Lesson 2
The history and evolution of doula work
From ancient birth rooms to modern hospital suites — the story hasn't changed as much as you'd think
Learning objectives
- Trace the origins and historical role of doulas and traditional birth attendants across cultures.
- Understand how the modern doula profession developed and became recognized in contemporary maternal care.
- Identify key social, cultural, and medical factors that have shaped the doula role over time.
Birth support is ancient — the job title is new
Here's a fun fact to open with: doulas are not a trend. The idea that a birthing person needs continuous, compassionate, non-medical support is literally as old as humanity. Across nearly every culture in recorded history, women did not give birth alone in a clinical room. They were surrounded by experienced women from their community — grandmothers, neighbors, midwives, wise elders — whose job was not to deliver the baby, but to hold the space around the person delivering it.
Archaeologists have found stone carvings and ancient artwork depicting women supporting other women in labor. Ancient Egyptian texts describe experienced birth attendants present at deliveries. The ancient Greeks had a name for the experienced women who assisted at births — and yes, it's where we get our word. Doúla in Greek meant "woman who serves." It was first applied to the modern professional role by medical anthropologist Dana Raphael in her 1973 book The Tender Gift: Breastfeeding, making her the first scholar to name something that had been happening for thousands of years.
Worth sitting with
The job existed for millennia before the word did. When you introduce yourself as a doula to a client from a culture with strong birth traditions, you are not offering them something foreign — you are offering a formalized version of something their great-great-grandmother probably already knew.
Three eras of birth support
Before 1900s
Community-centered birth
Birth happened at home, surrounded by experienced women. Support was relational, cultural, and continuous. No shift changes. No competing patients.
Early–mid 1900s
The medicalization gap
Birth moved to hospitals. Survival rates improved — but continuous personal support disappeared. Families were often excluded. Birthing people labored alone or with minimal contact.
1980s–today
The evidence-based revival
Research confirmed what grandmothers always knew. Continuous support improves outcomes. The professional doula was born — old wisdom in a new form.
What happened in the middle: the medicalization gap
By the early 20th century, birth had largely moved out of the home and into the hospital. This was, in many ways, a medical breakthrough — maternal and infant mortality fell significantly as sterile environments and skilled obstetric care became available. No one should romanticize the risks of pre-modern birth.
But something was also lost. The continuous, personal, relational support that had always surrounded birth got left behind. Hospitals ran on shifts. Nurses managed multiple patients. Families often waited in separate rooms. The birthing person — in one of the most intense experiences of their life — was suddenly far more isolated than any previous generation had ever been.
To picture it
Imagine going through something physically and emotionally enormous, with people rotating in and out every few hours, none of whom know your name well, your fears, or what you hoped your birth would feel like. That was the standard experience for decades. The modern doula exists to close that gap.
The research that changed everything
In the 1970s and 1980s, researchers Dr. John Kennell and Dr. Marshall Klaus began studying whether having a consistent, continuous support person during labor actually made a measurable difference. The results were striking. Women with continuous support had shorter labors, fewer interventions, and more positive birth experiences (Hodnett et al., 2013).
Their work asked — and answered — a simple question: does it matter if someone stays with you? Yes. Consistently and significantly. The 2017 Cochrane systematic review (Bohren et al.) later synthesized 27 randomized controlled trials across nearly 16,000 women and confirmed the same finding: continuous support from a trained doula produces better outcomes than any other form of support, or no support at all.
"Continuous labor support is a rare example of a healthcare practice found to have many benefits and no known harms."— Bohren et al., Cochrane Database of Systematic Reviews, 2017
This research gave the doula profession its scientific foundation — and its urgency. What communities had practiced intuitively for generations was now backed by rigorous evidence.
How DNT Network fits into this story
Where you come in
The Doulas and Nurturing Traditions Network (DNT Network) was built on exactly this premise — that honoring diverse cultural traditions of birth support and grounding that support in modern evidence are not competing goals. They are the same goal. The name itself reflects this: nurturing traditions are the ancient thread; the network is the modern infrastructure. DNT Network's training is available internationally, recognized by Medicaid programs and insurance providers, and designed by public health PhDs, OB/GYNs, and certified midwives — making evidence-based doula education accessible across all 50 states and over 100 countries.
When you complete this training, you are not entering a new field. You are entering a very old one — with better tools, a stronger evidence base, and a professional community to support you. That's the arc of this history: ancient practice, scientific validation, professional structure.
Scenarios & tips
Scenario 1
A pregnant client asks why they should hire a doula when the hospital already has nurses.
"That's a great question. Nurses are highly skilled at clinical care, but they're also managing monitoring, documentation, and often multiple patients at once. My role is different — I'm there from start to finish, focused entirely on your emotional comfort, physical support, and helping you understand your options. We're actually a team."
Tip: This response acknowledges nurses rather than competing with them — which is both accurate and builds trust with hospital staff you'll work alongside.
Scenario 2
A client from a cultural background with traditional birth attendants mentions that her grandmother was a "birth helper" at home.
"That's a beautiful tradition. In so many cultures, women have always supported each other through birth — that wisdom is real and it matters. What I do carries that forward in a modern setting. My role is to honor those traditions while also helping you navigate the hospital environment, so you feel held in both worlds."
Tip: Never position professional doula work as superior to cultural traditions. Position it as continuous with them. This builds immediate rapport and trust.
Scenario 3
A partner asks if doulas are just a "new trend."
"Actually, doulas are about as old as childbirth itself. What's new is the training and the professional recognition. For thousands of years, every culture had experienced women who supported births. What changed in the 20th century was that birth moved to hospitals — and that community support got left behind. Doulas exist to bring it back, in a form that works inside modern healthcare."
Tip: Framing doula work as historically grounded — not a wellness fad — builds credibility, especially with skeptical partners or family members.
🧠 Check your understanding
1
What was lost when birth moved from home to hospital in the early 20th century? Why didn't nurses fill that gap automatically?
2
How did the research of Klaus and Kennell in the 1970s–80s change the conversation around birth support? What did it prove that communities had always known intuitively?
3
The DNT Network name includes the phrase "nurturing traditions." Based on what you've read, why is honoring cultural birth traditions considered part of evidence-based doula practice — not separate from it?
References
- Bohren, M. A., Hofmeyr, G. J., Sakala, C., Fukuzawa, R. K., & Cuthbert, A. (2017). Continuous support for women during childbirth. Cochrane Database of Systematic Reviews, 7, CD003766. https://doi.org/10.1002/14651858.CD003766.pub6
- Hodnett, E. D., Gates, S., Hofmeyr, G. J., & Sakala, C. (2013). Continuous support for women during childbirth. Cochrane Database of Systematic Reviews, 7, CD003766. https://doi.org/10.1002/14651858.CD003766.pub5
- Raphael, D. (1973). The tender gift: Breastfeeding. Prentice-Hall. [First scholarly use of the term "doula"]
- DNT Network. (n.d.). About DNT Network. https://www.dntnetwork.com/about
- Morton, C. H., & Clift, E. (2014). Birth ambassadors: Doulas and the re-emergence of woman-supported birth in America. Praeclarus Press.
What is a doula?
Featured Study

The Effect of Doulas on Maternal & Birth Outcomes (2023)
The effect of doulas on maternal and birth outcomes: A scoping review. (2023). PMC10292163. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10292163/
Summary:
This scoping review looked across many studies to understand how doulas influence birth outcomes. It found that doula support is associated with fewer cesareans, shorter labor, and better breastfeeding success. Emotional support from doulas was linked to reduced stress and anxiety during childbirth. The review noted that doulas often help women feel more confident making decisions. Particularly for low-income women, doula involvement improved early breastfeeding and birth experience. The review suggests doulas may help close gaps in birth equity. It also acknowledged that access barriers exist and more research is needed to explore long-term maternal health.
What It Means to Birth Doulas:
For childbirth professionals, this review compiles consistent evidence that doula presence correlates with better physiological and emotional outcomes. It supports doulas’ role as a key part of person-centered support rather than an optional extra. The findings affirm doulas’ contributions to both physical and emotional well-being during birth. It also highlights the impact doulas can have for underserved communities. This reinforces the importance of culturally competent care. Doulas may be especially effective when incorporated early into prenatal planning. The data can help doulas demonstrate value to clients and care teams alike.
Translating for Doula Clients:
“Multiple studies show that continuous support through a doula is linked with less need for medical interventions and more satisfying birth experiences.”
Share evidence about emotional well-being: “Feeling calm and supported during labor isn’t just about comfort – research connects this support with positive outcomes like successful breastfeeding.”
Use language that validates their feelings and choices. Encourage them to think about the type of support they want. Reassure them that your work is rooted in research about maternal empowerment and resilience.
Unit 1 · Lesson 3
Distinguishing between a doula, midwife, and other birth professionals
Same room, very different jobs — and understanding the difference makes you better at yours
Learning objectives
- Differentiate the unique roles of doulas, midwives, obstetricians, and nurses in the childbirth process.
- Understand the non-clinical versus clinical responsibilities of birth professionals.
- Recognize how collaboration between doulas and medical providers improves outcomes for families.
Everyone is on the same team — playing different positions
Picture a birth room. There might be a nurse checking the monitor, a midwife reviewing progress, an OB/GYN on call down the hall, a partner gripping a hand — and a doula. To someone walking in, it can look like everyone is doing the same thing: supporting a person through labor. But the roles are profoundly different, and understanding exactly where each one begins and ends is one of the most important things you'll learn as a birth doula.
This isn't just useful for your own clarity. Research consistently shows that role confusion between doulas and clinical staff is one of the primary sources of tension in birth settings (Wójcik-Brylska et al., Midwifery, 2023). Knowing precisely what you do — and what you don't do — makes you a better collaborator, a safer practitioner, and a more trusted presence in the room.
A useful frame
Think of the birth team like an orchestra. The OB/GYN is the conductor — stepping in for complex moments, making high-stakes calls. The midwife is the lead musician — trained, clinical, directing the flow of birth. The nurse is the section player — skilled, essential, managing multiple instruments at once. And the doula? The doula is the one who stays next to the person performing, the whole time, making sure they feel supported enough to do what they came to do.
Meet the birth team
Non-clinical
Birth doula
Provides continuous emotional, physical, and informational support from early labor through the first hours postpartum. Does not perform medical tasks. Present for the entire birth experience — not shift-based.
Core focus: presence, comfort, communication
Licensed clinical
Certified nurse-midwife (CNM)
A licensed medical professional trained to provide full prenatal, labor, and postpartum care for low-risk pregnancies. Can monitor fetal heart tones, administer medications, and deliver babies. Practices in hospitals, birth centers, and homes.
Core focus: clinical management of normal birth
Physician
Obstetrician / OB-GYN
A medical doctor specializing in pregnancy, childbirth, and reproductive health. Manages high-risk pregnancies, performs cesarean sections, and handles surgical and emergency interventions. Typically arrives for delivery or complications.
Core focus: medical and surgical management
Licensed clinical
Labor & delivery nurse
A registered nurse who monitors vital signs, administers medications, and supports the clinical care team throughout labor. Typically manages multiple patients per shift. Research shows nurses spend only 6–10% of their time on direct labor support (Al-Adeli et al., 2025).
Core focus: clinical monitoring and procedures
Side-by-side: who does what
| Task / responsibility | Doula | Midwife | OB-GYN | L&D Nurse |
|---|---|---|---|---|
| Continuous presence during labor | Yes | No — episodic | No — on-call | No — shift-based |
| Delivers babies | No | Yes | Yes | No (emergencies excepted) |
| Administers medications | No | Yes | Yes | Yes (under orders) |
| Performs clinical exams | No | Yes | Yes | Yes |
| Cesarean sections | No | No | Yes | No |
| Emotional & comfort support | Yes — primary role | Yes — secondary | Yes — limited | Yes — limited |
| Prenatal relationship-building | Yes — weeks before | Yes | Yes | No |
| Makes medical decisions | No — never | Yes | Yes | Under supervision |
Why the doula's non-clinical status is a superpower
It's tempting to read "non-clinical" as a limitation. It isn't. A doula's freedom from clinical responsibilities is exactly what makes the role uniquely effective. Because a doula has no monitoring duties, no documentation requirements, no other patients, and no medical decisions to make, they can do something no one else in the room can: stay completely, undividedly present with one person for the entire arc of labor.
This is precisely what the research captures. The 2017 Cochrane systematic review (Bohren et al.) found that outcomes were strongest when support was provided by someone present solely to provide support — not a staff member with clinical duties, not a family member. The doula role is the only birth role defined by exclusion of clinical tasks, and that exclusion is the mechanism of its effectiveness.
Research: doulas and midwives together
A 2022 study published in eClinicalMedicine (The Lancet) found that women who received doula care alongside a midwife-led clinical team had the most consistent reductions in cesarean delivery — regardless of when doula care began. The study also found a 52.9% lower odds of cesarean delivery and a 57.5% lower odds of postpartum depression or anxiety among women who received doula support. These findings point not to competition between roles, but to the power of combining them. (Falconi et al., eClinicalMedicine, 2022)
The collaboration challenge — and how to navigate it
Research shows that when doula-midwife and doula-nurse collaboration works well, it creates what one Oxford qualitative study called a "team for the mother" — with doulas described as complementary colleagues who extended the care midwives could offer (McLeish & Redshaw, Midwifery, 2018). When it doesn't work well, the same study found that role confusion and unclear boundaries created friction.
An integrative review of doula-midwife collaboration published in Midwifery (Wójcik-Brylska et al., 2023) concluded that effective collaboration requires mutual understanding of each role's scope, and that doulas who clearly communicate their purpose and stay within their lane are far more likely to be welcomed as partners by clinical staff.
Where tension tends to arise
The most common friction points identified in research are: doulas perceived as contradicting clinical advice, doulas "speaking for" clients rather than helping them speak for themselves, and ambiguity about what the doula is there to do. The solution to all three is the same: clarity, humility, and genuine teamwork. You are not there to compete with anyone. You are there to fill the gap that everyone else — by virtue of their other responsibilities — structurally cannot fill.
"The doula will be the only person who is consistent. That is so valuable because she can bond with that person, and the doula can help her feel safe and supported."— Certified nurse-midwife, quoted in Exploring Innovative Models of Doula Services, PMC, 2024
Scenarios & tips
Scenario 1
A labor and delivery nurse seems irritated by your presence and says, "We've got it covered in here."
"Absolutely — you're doing an incredible job managing everything. I'm just here to provide the continuous emotional and physical support piece so that weight isn't falling on you. If there's anything I can do to make the room work better for everyone, please let me know."
Tip: Nurses are often stretched thin and sometimes misunderstand the doula role. Acknowledging their workload and clearly positioning your role as complementary — not competitive — tends to shift the dynamic quickly.
Scenario 2
Your client asks you whether she should accept the epidural her midwife is recommending.
"That's entirely your decision, and I'm here to support you whatever you choose. Would it help to ask the midwife a few questions first — like what the timing looks like, and what the alternatives are at this stage? I can be right here with you while you talk it through."
Tip: This is not your call to make — medically or personally. Your role is to help your client feel informed and empowered, not to steer the decision. Offering to facilitate the conversation with the midwife is exactly the right move.
Scenario 3
A family member asks why their loved one hired a doula when they already have a midwife and a great hospital team.
"That's a great question. The midwife and nurses are incredibly skilled — they're managing the clinical side of birth. What I do is different: I stay by her side the entire time, focused only on her comfort, her emotional experience, and making sure she feels heard. They work on the medical part; I work on the human part. It's actually most powerful when both are there."
Tip: Never position your role as replacing or compensating for a weak clinical team. Position it as the layer of support that clinical roles, by structural necessity, cannot provide — regardless of how excellent those providers are.
🧠 Check your understanding
1
In your own words, explain why a doula's non-clinical status is described as a structural advantage rather than a limitation. What does this allow a doula to do that no clinical provider can?
2
Research shows nurses spend only 6–10% of their time on direct labor support. Why does this gap exist — and how does understanding this help you work more effectively alongside nursing staff?
3
The Falconi et al. (2022) study found the strongest outcomes when doulas worked alongside midwife-led teams. What does this suggest about the relationship between doula support and clinical care?
4
A client's OB-GYN introduces a clinical recommendation your client hadn't anticipated. Walk through how you would support your client in that moment, being specific about what you would and would not do.
Peer-reviewed references
- Bohren, M. A., Hofmeyr, G. J., Sakala, C., Fukuzawa, R. K., & Cuthbert, A. (2017). Continuous support for women during childbirth. Cochrane Database of Systematic Reviews, 7, CD003766. https://doi.org/10.1002/14651858.CD003766.pub6
- Falconi, A. M., Bromfield, S. G., Tang, T., & Disciglio, R. (2022). Doula care across the maternity care continuum and impact on maternal health: Evaluation of doula programs across three states using propensity score matching. eClinicalMedicine (The Lancet), 50, 101531. https://doi.org/10.1016/j.eclinm.2022.101531
- McLeish, J., & Redshaw, M. (2018). A qualitative study of volunteer doulas working alongside midwives at births in England: Mothers' and doulas' experiences. Midwifery, 56, 53–60. https://doi.org/10.1016/j.midw.2017.10.002
- Wójcik-Brylska, K., Pawlicka, P., Tataj-Puzyna, U., Szlendak, B., Węgrzynowska, M., Pięta, B., & Baranowska, B. (2023). Cooperation between midwives and doulas in the context of perinatal care: An integrative review. Midwifery, 124, 103731. https://doi.org/10.1016/j.midw.2023.103731
- Al-Adeli, N., et al. (2025). Role of doulas across the pregnancy care continuum on maternal and child health: A scoping review. npj Women's Health. https://doi.org/10.1038/s44294-025-00109-4
- Exploring innovative models of doula services in maternity care: A qualitative study on advancing equity and addressing disparities. (2024). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC12144344/
- Tumblin, A., & Simkin, P. (2001). Pregnant women's perceptions of their nurse's role during labor and delivery. Birth, 28(1), 52–56. [Referenced via Al-Adeli et al., 2025 — nurses spend only 6–10% of time on labor support vs. 53% expected by patients]
Featured Study

Falconi, A. M., & colleagues (2022). Doula Care Across the Maternity Care Continuum.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9257331/
Summary:
This research evaluated doula programs across three U.S. states, focusing on maternal health outcomes using matched comparison methods. It found that women with doulas had lower odds of cesarean section and lower likelihood of postpartum depression or anxiety. The magnitude of these effects varied depending on the timing of support. The study also suggests doulas may help reduce disparities in outcomes for socioeconomically vulnerable and marginalized groups. It noted comprehensive evidence that doula involvement relates to improved maternal health, although more research is needed. Strengths of the study included reducing selection bias by using claim data and matched comparisons.
What It Means to Birth Doulas:
This study reinforces that doula care may improve both physical outcomes (like fewer cesareans) and emotional well-being after birth. It also underscores the importance of when doulas engage in care (early prenatal vs. only during labor). For doulas, this supports intentional integration of emotional support skills alongside physical comfort strategies. The findings also emphasize the role of doulas in health equity by supporting marginalized groups. It encourages doulas to document their impact and contribute to broader maternal health conversations.
Translating for Clients:
Use evidence to normalize the value of emotional support:
“Studies show that women with doulas had lower rates of cesarean birth and lower risk of anxiety or depression after birth.”
Help them connect expectations with care:
“Talking about your feelings and comfort needs early can make a real difference — and that’s part of what I’m here to support.”
Highlight continuity:
“We’ll work together from pregnancy through early postpartum so you feel supported at every stage.”
Module 1: Introduction to Birth Doula Work
Lesson 1.1 Quiz: What Is a Birth Doula?
Test your understanding of what a birth doula is, the history of doula work, and how doulas differ from midwives and other birth professionals. Select an answer for each question to see immediate feedback.
1. What is a birth doula?
✓ Correct! A birth doula is a trained, non-medical support person. The role is centered on continuous physical, emotional, and informational support — not clinical care.
✗ Not quite. Birth doulas are not medical professionals. They are trained companions who provide non-medical support throughout the childbirth journey.
2. Where does the word "doula" originate from?
✓ Correct! The word "doula" comes from ancient Greek, meaning "a woman who serves." It reflects the long tradition of women supporting other women through birth.
✗ Not quite. The term "doula" has Greek origins, meaning "a woman who serves" — pointing to the role's deep historical roots in serving birthing people.
3. Which of the following best describes the historical role of doulas across cultures?
✓ Correct! Women supporting other women in childbirth is one of the oldest traditions in human history, found across cultures worldwide — long before the modern doula movement was named.
✗ Not quite. Doula-like support has existed for centuries across many cultures — it is not a modern invention or limited to one region.
4. The modern doula movement, as we know it today, gained traction primarily in which decade?
✓ Correct! The modern doula movement took shape between the 1970s and 1990s, with research and formal training organizations developing during this period.
✗ Not quite. While doula-like roles existed for centuries, the modern doula movement and formal training programs emerged in the late 20th century.
5. What is the main difference between a birth doula and a midwife?
✓ Correct! This is the core distinction: midwives are medical care providers who can deliver babies and manage clinical care, while doulas offer non-medical, continuous support.
✗ Not quite. The key difference is scope: midwives are trained medical professionals, while doulas provide non-medical support.
6. Which of the following is NOT a role of a birth doula?
✓ Correct! Vaginal exams and fetal monitoring are clinical tasks performed by medical professionals — not doulas. Doulas stay within a non-medical support role.
✗ This is actually a valid doula role. Look for the option involving clinical or medical tasks — that's the one outside a doula's scope.
7. How does a birth doula typically work alongside a doctor or midwife?
✓ Correct! Doulas don't replace medical providers — they work alongside them, filling the gap with continuous emotional, physical, and informational support.
✗ Not quite. Doulas complement, rather than replace, clinical care. Their role is to support the birthing person while the medical team handles the clinical side.
8. True or False: A birth doula provides medical advice and clinical recommendations.
✓ Correct! Doulas do not give medical advice. They share information and resources, but clinical recommendations come from medical providers.
✗ Actually, false. Doulas may share information, but they do not give medical advice or make clinical recommendations — that's the role of doctors and midwives.
9. Which of the following best describes the type of support a doula provides?
✓ Correct! Doulas are known for their three-pronged support: physical (comfort measures), emotional (reassurance and presence), and informational (helping clients understand options).
✗ Not quite. The hallmark of doula support is its three-part nature: physical, emotional, and informational — all non-medical.
10. Which statement best summarizes what a birth doula is?
✓ Correct! That's the heart of birth doula work — trained, non-medical, continuous support that walks alongside the birthing person and their family before, during, and after birth.
✗ Not quite. A birth doula is trained (not untrained), non-medical (not clinical), and offers continuous support throughout pregnancy, birth, and postpartum.
-
A birth doula is a trained professional who provides continuous physical, emotional, and informational support to a birthing person before, during, and shortly after childbirth.
Doulas do not provide medical care but work alongside healthcare providers to enhance the birth experience.
-
Bohren, M. A., Hofmeyr, G. J., Sakala, C., Fukuzawa, R. K., & Cuthbert, A. (2017). Continuous support for women during childbirth. Cochrane Database of Systematic Reviews, 7, CD003766. https://doi.org/10.1002/14651858.CD003766.pub6
This Cochrane Review found that continuous labor support, often provided by doulas, leads to shorter labors, fewer cesareans, less need for pain medication, and greater maternal satisfaction.Steel, A., Frawley, J., Sibbritt, D., & Adams, J. (2015). Trained or professional doulas in the support and care of pregnant and birthing women: A critical integrative review. Health & Social Care in the Community, 23(3), 225–241. https://doi.org/10.1111/hsc.12112
This review examined professionalization of doulas, highlighting their unique role distinct from midwives and physicians, and how role clarity influences care experiences.McLeish, J., & Redshaw, M. (2018). A qualitative study of volunteer doulas working alongside midwives at births in England: Mothers’ and doulas’ experiences. BMC Pregnancy and Childbirth, 18, 35. https://doi.org/10.1186/s12884-018-1667-0
This study found that respectful collaboration between doulas and midwives improved women’s experiences, reduced stress, and enhanced communication in maternity care.Jordan, B. (1993).Birth in four cultures: A crosscultural investigation of childbirth in Yucatan, Holland, Sweden, and the United States (4th ed.). Prospect Heights, IL: Waveland Press.
Jordan’s anthropological work documents that birth support figures are a cross-cultural constant, embedding the doula role in human societies historically.Kennell, J. H., Klaus, M. H., McGrath, S. K., Robertson, S., & Hinkley, C. (1991). Continuous emotional support during labor in a US hospital: A randomized controlled trial. JAMA, 265(17), 2197–2201. https://doi.org/10.1001/jama.1991.03460170051032
This landmark RCT showed that continuous emotional support shortened labor, lowered cesarean rates, and reduced need for pain relief, sparking modern doula interest.Kozhimannil, K. B., Hardeman, R. R., Attanasio, L. B., Blauer-Peterson, C., & O’Brien, M. (2016). Doula care, birth outcomes, and costs among Medicaid beneficiaries. American Journal of Public Health, 106(4), 698–704. https://doi.org/10.2105/AJPH.2015.302982
This study found that Medicaid beneficiaries with doula support had lower odds of cesarean delivery, lower costs, and improved maternal satisfaction, especially among women of color.Gruber, K. J., Cupito, S. H., & Dobson, C. F. (2013). Impact of doulas on healthy birth outcomes. Journal of Perinatal Education, 22(1), 49–58. https://doi.org/10.1891/1058-1243.22.1.49
This study reported that doula care was associated with reduced anxiety, fewer symptoms of postpartum depression, and healthier maternal mental health. -
Falconi, A. M., Ramirez, L., & Levin, C. (2024). Role of doulas in improving maternal health and health equity among Medicaid enrollees, 2014–2023. 114(11):1275–1285. https://doi.org/10.2105/AJPH.2024.307805
Lay Summary:
This large U.S. study analyzed health insurance claims data comparing people with doula services to those without. It found 47% lower risk of cesarean delivery and 29% lower risk of preterm birth among those with doulas. Clients supported by doulas were also 46% more likely to attend postpartum checkups. These outcomes suggest doulas contribute to both physical health and healthcare engagement after birth. The research included matched pairs of Medicaid enrollees, meaning groups were comparable on key demographics. The study supports doulas as a strategy to reduce disparities in maternal health. It also noted the growing policy interest in dolua coverage.What It Means to Birth Doulas:
This evidence is powerful for doulas working with marginalized or low-income clients. It affirms that doula care is linked to significant reductions in common risks like cesareans and preterm birth. The increased likelihood of postpartum visits suggests doulas support holistic care continuity, not only during labor. For doulas, it’s a reminder to emphasize coordination with clinical teams. It also supports advocacy for broader doula access and insurance coverage. This study strengthens the argument that doulas contribute to health equity.Translating for Clients:
In consultations, you might say:“Research found that people with doula support had almost half the risk of cesarean delivery and had healthier timing of birth.”
Frame postpartum care as part of holistic support:
“People with doulas were more likely to go to their postpartum check-ups — that’s important for long-term health.”
This ties into empowerment and advocacy. Link evidence to their goals, e.g., “Let’s discuss how your preferences for birth and early support can shape your care plan.”