Module 1: Foundations of Human Lactation (20 hrs)
IN THIS LESSON
Introduction
Lactation is a coordinated system of structures, nerves, and hormones working together to make and move milk. In this lesson you’ll learn how the breast is built (alveoli, ducts, myoepithelial cells), how hormones like prolactin and oxytocin turn that hardware “on,” and how effective milk removal keeps the system running. We’ll connect normal physiology to everyday problems—engorgement, low transfer, nipple pain—so you can spot what’s off and choose the simplest fix. By the end, you’ll be able to explain why a deeper latch, skin-to-skin, or timely expression works—not just that it does.
The Anatomy & Physiology of Lactation
Understanding breast structure, milk synthesis, hormonal regulation, and the mechanics of milk release — the essential foundation for every lactation specialist.
In This Lesson
- Topic 1 — Breast Structure and Function: The anatomy of the breast and how each component contributes to lactation
- Topic 2 — Hormonal Regulation of Milk Production: The roles of prolactin, oxytocin, and other hormones in milk synthesis and release
- Topic 3 — The Letdown Reflex: The physiology of milk ejection and the factors that influence it
Every conversation you will ever have with a breastfeeding parent about milk supply, latch, pumping output, or feeding frequency begins with the same invisible foundation: the biology of the breast itself. Understanding how the breast is built, how it makes milk, and how it releases that milk under hormonal control is not academic background knowledge — it is the lens through which everything you observe in practice will make sense.
This lesson builds that foundation. We will move from the physical structures inside the breast, through the hormones that drive milk production and release, to the elegant reflex that sends milk to the baby. Along the way, we will connect every concept to what you will actually see and hear from the families you support.
Topic 1
Breast Structure and Function
The breast is a remarkably specialized gland — its entire architecture is organized around a single purpose: producing and delivering milk. Before the milk-making process can make sense, the physical layout needs to be clear.
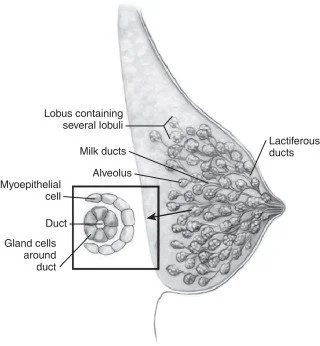
Think of the breast like a tree in winter, viewed from the side. The trunk is the nipple. Branching outward from it are a network of ducts, growing progressively smaller as they reach toward clusters of tiny grape-like structures at the very tips of the branches. Those clusters are where milk is actually made. Everything else in the breast — fatty tissue, connective tissue, blood vessels, nerves, lymph channels — exists to support that process and hold it all in place.
Figure 1.1 — Cross-section of the lactating breast showing the major structures involved in milk production and delivery. The alveoli (green clusters) are the milk-secreting units; milk travels through a branching duct system to reach the nipple.
The Key Structures, One at a Time
🍇 Alveoli
Tiny, sac-like structures surrounded by milk-secreting cells (lactocytes) and myoepithelial cells. This is where milk is actually produced. Each alveolus looks like a small hollow balloon lined with cells that draw nutrients from the bloodstream and convert them into breast milk components.
🌿 Lobules
A cluster of alveoli grouped together forms a lobule. Each breast contains many lobules arranged in 15–20 sections called lobes. Think of lobules as the grape clusters on a vine — multiple clusters make up one lobe.
🌊 Milk Ducts (Lactiferous Ducts)
Tube-like passages that carry milk from the lobules toward the nipple. The ducts converge and widen slightly as they approach the nipple, forming 4–18 openings at the surface. Older texts described "lactiferous sinuses" as milk reservoirs — current ultrasound research shows the ducts are more pipe-like than sac-like.
🔴 Myoepithelial Cells
Contractile cells that wrap around the outside of each alveolus like a tiny fist. When oxytocin signals them to squeeze, they compress the alveolus and push milk into the ducts. These are the cells responsible for the letdown reflex — without them, milk made inside the alveoli would stay there.
🔵 Lactocytes
The milk-secreting cells lining the inside of each alveolus. They pull water, glucose, amino acids, fatty acids, and immune factors from nearby capillaries and assemble them into the complex fluid we call breast milk. Prolactin is their main activating hormone.
🩷 Nipple & Areola
The nipple is the delivery point — where 4–18 lactiferous duct openings release milk to the baby. The areola contains Montgomery glands (the small bumps around the nipple) which secrete an oily substance that lubricates, protects, and helps the baby locate the breast by scent.
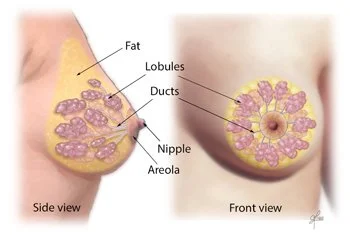
🧩 Adipose (Fatty) Tissue
The breast is largely composed of adipose tissue, which gives it its shape and size. Breast size has almost no relationship to milk-producing capacity — the glandular tissue (alveoli, lobules, ducts) determines supply potential, not the volume of fat surrounding it.
🔗 Cooper's Ligaments
Fibrous bands that run from the chest wall through the breast to the skin, providing structural support. They are not involved in milk production, but understanding them helps explain why breast fullness and engorgement can cause discomfort — the ligaments stretch under increased tissue pressure.
Breast Size and Supply: Setting the Record Straight
One of the most persistent myths in lactation is that breast size determines milk-making capacity. It does not. Milk-producing capacity is determined by the amount of glandular tissue (alveoli and lobules), not by breast size or cup size. A parent with small breasts can have abundant glandular tissue and produce a full milk supply. Similarly, a parent with large breasts may have relatively less glandular tissue. Breast size is almost entirely determined by adipose tissue volume, which has no role in milk synthesis.
When counseling families, this distinction is practically important: a parent worried that her small breasts cannot "make enough milk" needs factual reassurance, not vague encouragement. The biology is on her side.

Early skin-to-skin contact and frequent feeding in the first days directly stimulate glandular tissue activity and hormonal pathways that establish milk supply.
How the Breast Changes Across the Life Cycle
The breast is not a static structure. It changes dramatically across puberty, pregnancy, the postpartum period, and weaning — and understanding these changes helps you counsel families about what to expect at each stage.
| Life Stage | What's Happening in the Breast | What This Means for Lactation |
|---|---|---|
| Puberty | Estrogen drives ductal growth; adipose tissue accumulates; the basic ductal framework forms | Baseline structure is established; full glandular development has not yet occurred |
| Pregnancy — 1st & 2nd Trimester | Prolactin, estrogen, and progesterone drive massive growth of lobular-alveolar tissue; milk ducts branch and multiply | Most of the milk-making infrastructure is built during pregnancy, well before birth |
| Pregnancy — 3rd Trimester | Lactocytes begin producing colostrum; progesterone suppresses active milk secretion | Colostrum is ready before birth; progesterone keeps the "tap" off until delivery |
| Birth — Days 1–3 (Lactogenesis II) | Delivery of placenta causes a dramatic drop in progesterone; prolactin surges; copious milk production begins | Milk "coming in" — often reported as breast fullness, warmth, or engorgement around days 2–5 |
| Established Lactation | Supply regulated by demand: frequent milk removal keeps prolactin receptors active and prevents involution | The foundation of supply-and-demand: milk that stays in the breast signals reduced production |
| Weaning | Reduced milk removal triggers apoptosis (cell death) in alveolar tissue; breast gradually involutes | Abrupt weaning risks engorgement and mastitis; gradual weaning is more comfortable |
Topic 2
Hormonal Regulation of Milk Production
The breast does not act alone. Milk production is orchestrated by a sophisticated team of hormones that communicate between the brain, the pituitary gland, the ovaries, the placenta, and the breast tissue itself. Understanding these hormonal signals is essential — because when milk supply is a concern, the answer almost always lies somewhere in this signaling chain.
The four hormones you need to know well for this course are prolactin, oxytocin, estrogen, and progesterone. Each plays a distinct role, and their interplay across pregnancy and postpartum is what makes lactation possible.
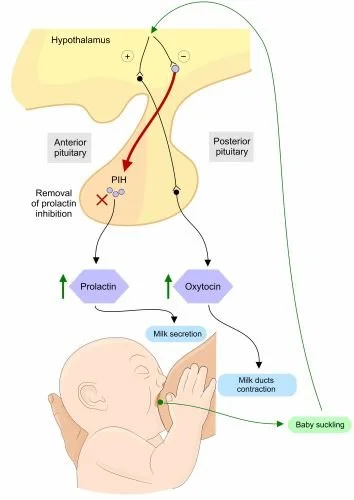
Prolactin
The primary milk-making hormone. Released from the anterior pituitary after nipple stimulation. Signals lactocytes to synthesize milk. Rises with each feeding; peaks about 30–45 minutes after the feeding begins. Often called the "milk-production hormone."
Oxytocin
The milk-release hormone. Released from the posterior pituitary and causes myoepithelial cells to contract and squeeze milk out of the alveoli. Triggered by suckling, baby's smell or cry, or psychological readiness. Often called the "love hormone."
Estrogen
Drives ductal growth during puberty and pregnancy. High estrogen during pregnancy promotes the physical growth of the breast's duct system. Postpartum estrogen remains low during exclusive breastfeeding — one reason menstrual cycles are often delayed.
Progesterone
The "inhibitory" hormone during pregnancy. Suppresses active milk secretion despite fully developed glandular tissue. Its dramatic drop after placental delivery is the signal that triggers copious milk production — this is why retained placental fragments can delay milk coming in.
Figure 1.2 — The hormonal pathway from nipple stimulation to milk production (prolactin, green pathway) and milk ejection (oxytocin, gold pathway). Both pathways are triggered simultaneously by suckling.
Lactogenesis: The Stages of Milk Coming In
Lactogenesis is the process by which the breast begins and establishes milk secretion. It unfolds in stages, and understanding these stages is directly relevant to the clinical conversations you will have with new parents — especially about timing, the difference between colostrum and mature milk, and what "milk coming in" actually means.
Real-World Example
Mara is a first-time parent who gave birth 36 hours ago. She calls her lactation specialist, Dani, in tears: "My baby keeps wanting to feed all the time. I can only express a few drops. My mother says my milk hasn't come in and my baby is starving." Dani knows that what Mara is describing is perfectly normal. Mara's breasts are producing colostrum — a small but extremely concentrated, nutrient-rich substance that is precisely calibrated to a newborn's tiny stomach. The infant's frequent nursing is exactly what will stimulate Mara's prolactin and help transition her supply to mature milk over the next 24–72 hours. Dani helps Mara understand this distinction, offers reassurance backed by the biology, and outlines the signs that would indicate the baby is receiving enough colostrum.
| Stage | Timing | What Happens | Clinical Notes |
|---|---|---|---|
| Lactogenesis I | Mid-pregnancy (approx. 16 weeks) onward | Lactocytes differentiate and begin producing colostrum; progesterone suppresses full secretion | Some parents leak colostrum during pregnancy — this is normal |
| Lactogenesis II | Days 2–5 postpartum | Progesterone drops sharply after placenta delivery; prolactin surges; copious milk production begins; colostrum transitions to transitional milk, then mature milk | "Milk coming in" — associated with breast fullness, warmth, engorgement. Delay beyond day 5 warrants attention (retained placenta, hormonal issues, insufficient removal) |
| Lactogenesis III (Galactopoiesis) | Day 9 onward (established lactation) | Supply regulated by demand — autocrine (local) control via feedback inhibitor of lactation (FIL); frequent milk removal maintains supply | This is the supply-and-demand phase. Missed or delayed feedings reduce supply; frequent removal increases it |
The Feedback Inhibitor of Lactation (FIL)
Once established lactation is underway, the body shifts from hormonal control (prolactin-driven) to a more localized, autocrine control system. The key player here is a whey protein called the Feedback Inhibitor of Lactation (FIL).
Here is the elegant logic: FIL is produced by the lactocytes and accumulates in the alveolus alongside the milk. When milk sits in the breast undrained, FIL concentration rises and signals the lactocytes to slow down production. When milk is removed frequently, FIL is drained away with it, and the lactocytes receive the signal to keep producing.
Why This Matters in Practice
FIL explains the single most important principle in supply management: milk removal drives milk production. The breast is not a passive container — it is an active, responsive system. Every time milk is removed — whether by a nursing baby, a pump, or hand expression — the breast receives the chemical signal to make more. Every time milk sits in the breast, the signal is "slow down."
This is why supplementing with formula without pumping or nursing can reduce supply. It is why pumping after a feeding, even briefly, can build supply. And it is why skipping nighttime feeds often leads to a gradual supply drop. The biology is consistent and logical — once you understand it, you can explain it clearly to families and troubleshoot supply concerns with confidence.
Hands-On Tip: Explaining FIL to a Parent
When parents ask why they need to nurse or pump so frequently, a simple analogy helps: "Your breast works a bit like a kitchen order system. When orders keep coming in — when milk keeps getting removed — the kitchen keeps cooking. When the orders stop coming, the kitchen slows down and eventually closes for the night. Frequent removal is how you keep the kitchen open."
Analogies like this make the science feel concrete and empowering rather than clinical and overwhelming.
Topic 3
The Letdown Reflex
You can have a breast full of milk and a baby perfectly positioned at the breast — but if the letdown reflex does not fire, the milk will not flow. Understanding the letdown reflex is essential to supporting families when feedings feel frustrating, unproductive, or painful.
The milk ejection reflex (letdown) is triggered by oxytocin. Here is the sequence in plain language:
1
Stimulus is detected
Baby latches and begins suckling. The nerve endings in the nipple and areola send sensory signals up to the hypothalamus in the brain. This can also be triggered by hearing a baby cry, thinking about the baby, or smelling the baby — the brain does not require physical contact to initiate the reflex.
2
Hypothalamus signals the posterior pituitary
The hypothalamus prompts the posterior pituitary gland to release oxytocin into the bloodstream. This is the same oxytocin involved in uterine contractions, bonding, and feelings of warmth and calm — which is why many parents report feeling relaxed or even drowsy during nursing.
3
Oxytocin reaches the breast
Circulating oxytocin reaches the myoepithelial cells surrounding the alveoli in the breast. These contractile cells respond rapidly — typically within 30–90 seconds of the start of feeding, though timing varies between individuals.
4
Myoepithelial cells contract
The myoepithelial cells squeeze the alveoli, propelling milk into the ducts. This creates a positive pressure wave through the duct system. If milk is abundant or pressure is high, some parents notice spraying or dripping from the opposite breast simultaneously.
5
Milk flows to the nipple
Milk moves through the converging duct system and out through the lactiferous duct openings at the nipple. Most feedings involve multiple letdowns — typically 2–4 per session — as the oxytocin level pulses in waves throughout the feeding.
What Letdown Feels Like — and What It Doesn't
One of the most common points of confusion for new parents is not knowing whether they have experienced a letdown. The sensory experience varies enormously between individuals, and it often changes over time.
✅ Common Letdown Sensations
Tingling or "pins and needles" in the breast, a sensation of fullness that suddenly releases, mild cramping (especially in the early postpartum period due to oxytocin's effect on the uterus), visible milk dripping or spraying from the breast, a change in the baby's sucking rhythm to slower, deeper swallows with audible gulping.
⚠️ When Parents Report Not Feeling It
Many parents — particularly those who are well-hydrated and experienced — report feeling little or nothing during letdown. This does not mean letdown is not occurring. If the baby is swallowing well and gaining weight appropriately, letdown is working even if the parent has no subjective sensation of it.
What Inhibits Letdown
The letdown reflex is exquisitely sensitive to psychological and physiological state. Adrenaline (epinephrine) — the stress hormone — is the primary antagonist of oxytocin. When a parent is stressed, anxious, in pain, embarrassed, or feeling unsafe, adrenaline suppresses the release of oxytocin, making letdown slower, less forceful, or absent.
Why Emotional State Is Not "Just Psychological"
When a parent says, "I just can't seem to let down when I pump at work," this is not a mindset problem — it is a physiological one. The work environment triggers stress hormones that directly compete with the oxytocin needed for milk ejection. This is why pump efficiency often drops in stressful environments, even when the same parent has no problem letdown at home.
Practical strategies include: looking at a photo or video of the baby, smelling a worn item of the baby's clothing, practicing a brief breathing or relaxation exercise before pumping, using a hands-free pump to reduce physical discomfort, and — where possible — advocating for a private, comfortable pumping space at work. Each of these interventions has a direct physiological rationale: they reduce adrenaline and support oxytocin release.

Skin-to-skin contact immediately after birth promotes oxytocin release, which supports both milk ejection and the emotional bond between parent and infant.
Factors That Support vs. Inhibit the Letdown Reflex
| Factor | Supports Letdown ✅ | Inhibits Letdown ⚠️ |
|---|---|---|
| Psychological state | Relaxed, confident, feeling safe and supported | Anxious, stressed, embarrassed, in pain, or feeling observed/judged |
| Sensory cues | Baby's scent, sight, or cry; warm compress on breast; familiar environment | Noisy or unfamiliar environment; discomfort; poor latch causing pain |
| Hydration & nutrition | Adequate fluid intake; balanced nutrition | Significant dehydration; severe caloric restriction |
| Physical factors | Good latch with effective milk transfer; comfortable positioning | Nipple pain; flat/inverted nipples without compensatory strategy; engorgement preventing effective latch |
| Hormonal factors | Normal postpartum prolactin and oxytocin levels | Certain medications; thyroid disorders; retained placenta affecting progesterone drop; stress-induced cortisol elevation |
| Pumping context | Private, comfortable setting; baby photos available; routine established | Workplace stress; shared/uncomfortable pump room; incorrect flange size |
Hands-On Tip: The Warm Compress Technique
For parents who struggle with letdown — especially when pumping — a warm, damp cloth applied to the breast for 2–3 minutes before nursing or pumping can significantly improve results. Warmth promotes vasodilation in breast tissue and stimulates nerve receptors associated with the letdown reflex. This is especially useful for:
- Parents returning to work who pump in stressful environments
- Parents dealing with engorgement, where a hard breast is difficult for the baby to latch onto
- Parents who are anxious about milk output and need a concrete, calming action to take before sessions
The technique costs nothing, carries no risk, and has a clear physiological rationale. It is one of the most reliable, accessible tools in a lactation specialist's toolkit.

An effective latch is the starting point for the entire hormonal cascade — each suckling event sends a nerve signal that triggers both prolactin (for milk synthesis) and oxytocin (for milk ejection).
Synthesis
Putting It All Together: Anatomy Meets Physiology in Practice
The three topics in this lesson are not separate islands of knowledge — they form an integrated system. The anatomy provides the hardware; the hormones provide the operating software; and the letdown reflex is the trigger that makes the whole system run in real time, feeding after feeding.
The Lactation Loop: How It All Connects
Baby latches effectively → nerve signals travel to the hypothalamus → prolactin released (lactocytes make milk) → oxytocin released (myoepithelial cells contract) → milk ejected into ducts → milk removed from the breast → FIL drained away → signal to keep producing is maintained → supply is sustained.
Every link in this chain matters. As a lactation specialist, your job is to identify which link is under stress when a family comes to you with a concern — and to apply your knowledge of the anatomy and physiology to figure out why, and what to do about it.
- Milk supply concern? Look at removal frequency (FIL), hormonal history (progesterone, thyroid), and glandular development
- Letdown problem at the pump? Look at stress factors, environment, flange fit, and psychological cues
- Milk "not coming in" by day 4–5? Consider retained placental tissue, birth history, and frequency of milk removal
- Pain with feeding? Examine latch quality (affects oxytocin inhibition), nipple anatomy, and oral function
📝 Knowledge Check
1. A parent tells you she has very small breasts and is worried she won't be able to make enough milk. What is the most accurate and reassuring thing you can tell her, and why?
Key Points Breast size is determined primarily by adipose (fatty) tissue, which has no role in milk production. Milk-making capacity depends on the volume of glandular tissue — alveoli, lobules, and ducts — which cannot be assessed by breast size or cup size. Most parents with small breasts have fully adequate glandular tissue and can produce a complete milk supply. She should be encouraged to begin feeding frequently after birth to establish supply through the demand-driven prolactin pathway.
2. Explain in plain language why a parent who starts supplementing with formula without pumping or feeding might notice their milk supply decreasing over the following week.
Key Points When formula replaces a breastfeeding session, milk is not removed from the breast during that window. As milk accumulates in the alveoli, Feedback Inhibitor of Lactation (FIL) builds up alongside it. Rising FIL concentration signals the lactocytes to reduce production. The less frequently milk is removed, the more FIL accumulates, and the lower supply becomes. This is not a malfunction — it is the body accurately responding to what it perceives as reduced demand.
3. A parent who has been pumping successfully at home returns to work and finds her pump output drops significantly despite following the same pumping schedule. What physiological explanation would you offer, and what practical strategies might help?
Key Points The work environment likely triggers a stress response (adrenaline/cortisol release) that suppresses oxytocin and inhibits the letdown reflex. This is a physiological, not psychological, problem. Strategies include: using a photo or video of the baby; smelling a worn baby item; applying a warm compress to the breast before pumping; creating a calming pre-pump routine; ensuring a private, comfortable pumping space; confirming correct flange size; and practicing brief relaxation techniques. Each of these directly supports oxytocin release.
4. What is Lactogenesis II, when does it typically occur, and what hormonal change triggers it?
Key Points Lactogenesis II is the onset of copious (high-volume) milk production, typically occurring between days 2–5 postpartum. It is triggered by the dramatic drop in progesterone that follows delivery of the placenta. With progesterone's inhibitory effect removed, prolactin surges and drives lactocytes to transition from colostrum to transitional and then mature milk production. Delay beyond day 5 may indicate retained placental fragments, hormonal disruption, or insufficient early milk removal.
References
-
Geddes, D. T. (2007). Inside the lactating breast: The latest anatomy research. Journal of Midwifery & Women's Health, 52(6), 556–563.
https://doi.org/10.1016/j.jmwh.2007.05.004 - Hartmann, P. E., Mitoulas, L. R., & Sherriff, J. L. (1998). Breastfeeding: The biological and physiological basis. In Breastfeeding and Human Lactation (2nd ed.). Jones and Bartlett.
-
Kent, J. C., Mitoulas, L. R., Cregan, M. D., Ramsay, D. T., Doherty, D. A., & Hartmann, P. E. (2006). Volume and frequency of breastfeedings and fat content of breast milk throughout the day. Pediatrics, 117(3), e387–e395.
https://doi.org/10.1542/peds.2005-1417 -
Neville, M. C., Morton, J., & Umemura, S. (2001). Lactogenesis: The transition from pregnancy to lactation. Pediatric Clinics of North America, 48(1), 35–52.
https://doi.org/10.1016/s0031-3955(05)70284-4 -
Pang, W. W., & Hartmann, P. E. (2007). Initiation of human lactation: Secretory differentiation and secretory activation. Journal of Mammary Gland Biology and Neoplasia, 12(4), 211–221.
https://doi.org/10.1007/s10911-007-9054-4

❋
Key Topics in Depth
1. Breast Structure and Function
Learning Objectives
Describe the main parts of the breast involved in lactation.
Explain how breast structures work together to produce and deliver milk.
Recognize normal breast changes during pregnancy and postpartum.
Definition & Explanation
The breast is not just “one organ,” but a system of different tissues working together to produce and deliver milk. The milk-making tissue is organized into lobes, which are like the slices of an orange. Each lobe is made up of lobules, and inside those lobules are tiny sacs called alveoli. These alveoli are the “milk factories” where breastmilk is made.
Milk flows out of the alveoli through small tubes called ducts, which connect to the nipple. Think of ducts as a system of straws that carry milk from where it’s made to where the baby can drink it. Around the nipple is the areola, which contains small glands that release oils to keep the nipple skin healthy and to provide a scent that helps guide newborns to latch.
During pregnancy, hormones like estrogen and progesterone signal the breast to grow more alveoli and ducts. This explains why breasts often feel fuller, heavier, or more tender in pregnancy. After birth, another hormone, prolactin, takes over as the main driver of milk production.
Example: Imagine the breast as a tree. The alveoli are the leaves where “milk” is made, the ducts are the branches that carry the milk, and the nipple is the trunk where everything comes together for the baby.
Scenarios & Tips
Scenario: A parent says, “Why do my breasts feel lumpy when they’re full?”
Response: “That’s normal. The lumps are the milk-filled lobules and alveoli. Once your baby nurses or you express milk, they’ll feel softer.”
Tip: Normalize fullness and changes—help parents recognize what’s expected vs. when to seek help (e.g., painful hard lumps).Scenario: A pregnant parent asks, “Why are my nipples darker than before?”
Response: “During pregnancy, the areola gets darker to help your baby see and find the breast more easily after birth.”
Tip: Use this as an opportunity to explain how the body naturally prepares to guide infants.Scenario: A parent says, “I don’t feel much breast change in pregnancy—should I be worried?”
Response: “Every body is different. Some people notice big changes, while others notice very little. It doesn’t necessarily mean you won’t make milk.”
Tip: Reassure without overpromising, and suggest follow-up if concerns continue postpartum.
Evidence-Based Insights
Recent evidence shows that what matters for milk production is function, not appearance. A large review by Geddes and colleagues reports that measured 24-hour milk production in lactating parents was not correlated with breast glandular tissue estimates, duct number/diameter, or storage capacity—meaning breast size/shape alone doesn’t predict supply. Practically, milk output is driven by effective, frequent removal and the lactation physiology that supports it. This helps families reframe concerns about “small” or “large” breasts and focus instead on latch quality, milk transfer, and feeding patterns. PMC
Another line of research explains why the areola matters for early feeds. In a PLOS ONE experiment, two-day-old newborns exposed to natural secretions from Montgomery (areolar) glands showed stronger breathing and mouth movements than to human milk, formula, or control odors—evidence that areolar scents act like a built-in “guidance system” that helps babies orient and begin feeding. This supports common best practices such as skin-to-skin care, early breast contact, and avoiding strong fragrances on the breast during the early postpartum period so those cues aren’t masked. PMC
Suggestions for lactation specialists
Reassure clients that breast size doesn’t predict supply; center your assessment on latch, transfer, infant output, and feeding frequency/response to demand. PMC
Coach frequent, effective milk removal (direct breastfeeding or well-fitted pumping) as the primary lever for protecting/boosting supply. PMC
In the first days, encourage uninterrupted skin-to-skin and early breast contact; advise avoiding perfumes/strong soaps on the breast to preserve areolar scent cues. PMC
When troubleshooting early latching, use positioning that lets the baby’s nose/cheeks contact the areola (baby-led latch), leveraging innate olfactory orientation. PMC
Key Terms & Definitions
Alveoli: Alveoli are tiny, grape-like sacs inside the breast where breastmilk is made and stored before it is released. These sacs are surrounded by specialized cells that produce milk in response to the hormone prolactin. When the letdown reflex is triggered, the muscles around the alveoli contract and push milk into the ducts. For example, you can think of alveoli as “mini milk factories” working nonstop to produce nourishment for the baby. The number and efficiency of alveoli can influence how much milk a parent produces. They are the starting point of the milk production and flow process.
Lobes/Lobules: Lobes and lobules are groups of alveoli that are organized in clusters, much like the sections of an orange. Each breast has multiple lobes, and inside each lobe are smaller lobules filled with milk-producing alveoli. This organization helps distribute milk production evenly across the breast. For instance, if one lobe is drained well during feeding, the body gets the signal to keep making milk in that area. This structure ensures that milk is available throughout the breast and not just from one part. Understanding this setup helps explain why it is important to switch sides or adjust positioning during breastfeeding.
Ducts: Ducts are the narrow tubes that carry milk from the alveoli, through the breast, and to the nipple where the baby can access it. They function like small pipelines, ensuring that milk produced deep inside the breast can reach the surface. When the milk ejection reflex is triggered, milk travels quickly through these ducts. For example, if a baby unlatches during letdown, milk might spray from the nipple, which is a sign of ducts releasing milk under pressure. Keeping ducts free of blockages is important, since clogged ducts can cause pain or even lead to infection. They are the “delivery system” of breastfeeding.
Areola: The areola is the darker, circular area around the nipple that contains glands and scent markers to guide the baby during feeding. These glands secrete oils that moisturize the skin and help prevent dryness or cracking. Babies are naturally drawn to the scent of the areola, which helps them find the nipple and latch effectively. For instance, even newborns placed skin-to-skin with their parent often crawl toward the breast, guided partly by the scent from the areola. Its color contrast also makes the nipple more visible to the baby. This area plays both a biological and sensory role in successful breastfeeding.
Prolactin: Prolactin is the hormone that drives milk production in the alveoli. Its levels rise after birth and continue to rise every time milk is removed, whether through breastfeeding or pumping. For example, when a baby nurses frequently during growth spurts, prolactin helps the body increase milk supply to meet demand. Without enough stimulation, prolactin levels drop, and milk production slows down. This hormone also contributes to a calming effect, helping parents feel more relaxed during feeding. It works hand-in-hand with oxytocin, ensuring both milk production and milk release.
FAQs: How Breast Structure Supports Milk Production
-
Scenario: A parent notices the left breast feels fuller and pumps more milk than the right.
Answer: It’s very common for one breast to be more productive. Differences in milk-making tissue, duct size, or how baby latches on each side can affect output. Both breasts still contribute to supply. As long as baby is gaining weight well, the imbalance isn’t harmful. -
Scenario: A parent feels small, movable lumps after a feed and worries about clogged ducts.
Answer: After feeding, you may feel small areas of firmness where lobules are located. These usually soften as milk is drained. If a lump persists, becomes painful, or is accompanied by redness or fever, that’s when to get checked. -
Scenario: A parent notices small raised spots on the areola during pregnancy.
Answer: Those are Montgomery glands—normal oil-producing glands that secrete substances to protect the nipple and help guide your baby to the breast. They’re not clogged pores and don’t need to be squeezed or treated. -
Scenario: A parent worries that flatter nipples won’t work for breastfeeding.
Answer: Babies don’t just latch to the nipple, but to the areola as well. Flat or inverted nipples can still work, especially with skin-to-skin, hand expression, and proper positioning. If baby struggles to latch, a lactation consultant can suggest techniques or tools like nipple shields. -
Scenario: A parent with smaller breasts is worried about not having enough milk for their newborn.
Answer: Breast size is determined mostly by fatty tissue, not the number of milk-making glands. Milk production depends on how often and effectively milk is removed, not breast size. Parents with small or large breasts can all make enough milk.
Breast anatomy and lactation
2. Hormonal Regulation of Milk Production
Definition & Explanation
Milk production and release depend on two key hormones: prolactin and oxytocin.
Prolactin is often called the “milk-making hormone.” It tells the alveoli (milk sacs) to produce milk. Prolactin levels rise when the baby suckles or when milk is removed by pumping or hand expression. The more milk is removed, the more prolactin signals the breast to make more—this is why frequent feeding helps supply.
Oxytocin is known as the “love hormone.” It triggers the muscle cells around the alveoli to contract, pushing milk down the ducts toward the nipple. This process is called the letdown reflex (covered in Topic 3). Oxytocin release can be influenced by emotions, touch, and relaxation.
Other hormones—like estrogen and progesterone—play major roles during pregnancy but decrease after birth, allowing prolactin and oxytocin to take over.
Example: Imagine a factory. Prolactin is the manager who tells the workers (alveoli) to produce more milk. Oxytocin is the shipping department that moves the product (milk) out of the factory and into the delivery trucks (ducts).
Scenarios & Tips
Scenario: A parent says, “I’m worried my milk supply is low because my baby is always nursing.”
Response: “Frequent nursing actually stimulates prolactin and helps build supply. Babies often cluster-feed to tell your body to make more milk.”
Tip: Reframe frequent feeding as a normal and healthy sign of hormonal regulation.Scenario: A parent says, “I feel tense, and milk doesn’t come out as easily—why?”
Response: “Stress can block oxytocin, which controls milk release. Relaxation, deep breathing, and skin-to-skin can help.”
Tip: Teach quick stress-relief tools that parents can use before or during feeding.Scenario: A parent asks, “Do I need special foods or supplements to increase prolactin?”
Response: “The most effective way to boost prolactin is frequent milk removal. Foods and teas can support you, but nursing and pumping are the most important drivers.”
Tip: Keep advice evidence-based—encourage demand-driven feeding over supplements as a first step.
Evidence-Based Insights
In a study by Uvnäs-Moberg et al. (2020), researchers conducted a systematic review of how oxytocin and prolactin respond during breastfeeding in human mothers. They found that oxytocin is released in pulsatile bursts in response to infant suckling (with peaks often within minutes), and that a greater number of oxytocin pulses early in lactation was associated with higher milk yield and longer duration of breastfeeding. However, they also observed that stressors (e.g. noise, mental stress) tend to reduce the number of oxytocin pulses during breastfeeding, which could blunt the milk ejection reflex (i.e. the “let-down”) and thereby reduce effective milk transfer (fewer pulses → less efficient ejection). In the same review, the authors noted that prolactin levels also rise during breastfeeding (usually gradually, over tens of minutes) and that oxytocin and prolactin responses are interconnected: oxytocin release seems to help promote physiological states (lower cortisol, calmer autonomic balance) that may support sustained lactation and maternal adaptation. In summary: the “spike after each feeding” claim is partly supported (prolactin does rise in response to feeding), but the relationship is more nuanced (timing, pulsatility of oxytocin matters, and stress can dampen that). (Uvnäs-Moberg et al., 2020) PLOS
A more recent empirical study by Nagel et al. (2021) examined how maternal psychological distress (stress, anxiety, depression) relates to lactation outcomes, and they reviewed mechanistic evidence about how stress may interfere with oxytocin and milk ejection. Their summary showed that higher levels of maternal distress are associated with delayed secretory activation (i.e. later onset of full milk “coming in”) and shorter duration of exclusive breastfeeding. One proposed mechanism is that psychological distress interferes with oxytocin release during infant suckling, thereby impairing the milk ejection reflex. If milk ejection is repeatedly weak or delayed, the breast may not be fully emptied, which in turn can lead to reduced milk production over time (since milk removal is a key driver of supply). They also note that maternal distress correlates with elevated cortisol and metabolic shifts (e.g. insulin resistance) which may have downstream effects on lactation physiology. Thus, the original idea that stress “interferes with oxytocin release” is well supported in this more recent review of human lactation data. (Nagel et al., 2021) PMC
Suggestions for lactation specialists:
Recognize that optimal oxytocin pulsatility and timing matter—not just the presence of hormone rise. Encourage feeding environments that reduce disturbance or anxiety (quiet, calm, supportive) to help maintain robust oxytocin release.
Monitor for signs that let-down is weak or delayed (baby fussing, long pauses before milk flows), and intervene early (positioning, breast massage, hands-on pumping) to assist the reflex.
Screen for maternal psychological distress (stress, anxiety, depression) early in the postpartum period, because elevated distress can impair oxytocin dynamics and thus milk ejection, which over time can affect supply.
Use interventions that support maternal mental well-being (emotional support, mindfulness, counseling referrals, peer support) as part of the lactation care plan—not just focusing on mechanical aspects.
Emphasize frequent, effective breast emptying especially in the first days, because even if hormonal responses are impaired, mechanical removal is still the key driver of maintaining supply.
Key Terms & Definitions
Prolactin: Prolactin is the main hormone responsible for stimulating milk production in the breasts. After birth, when the placenta is delivered, prolactin levels rise, signaling the body to begin producing milk. Every time a baby nurses or milk is removed, prolactin levels increase to encourage more milk production. For example, a mother who breastfeeds frequently will naturally produce more prolactin, helping her body maintain a steady milk supply. This is why consistent nursing or pumping is so important for keeping up with the baby’s needs. Prolactin works behind the scenes, ensuring that the milk supply is always ready.
Oxytocin: Oxytocin is often called the “love hormone” because it is linked with bonding and emotional connection, but it also plays a crucial role in breastfeeding. It is the hormone that triggers the letdown reflex, causing milk stored in the breast to flow out through the ducts. This can happen when the baby latches or even when a parent hears their baby cry. For example, some mothers notice milk leaking at the sound of their baby’s voice—this is oxytocin at work. Beyond milk release, oxytocin also helps the parent feel calmer and more connected to their baby during feeding. This hormone makes breastfeeding both a physical and emotional experience.
Supply-Demand Cycle: The supply-demand cycle describes how the body makes milk in response to how often and how much milk is removed. The more frequently the baby nurses or milk is pumped, the more milk the body is signaled to produce. For example, a parent who breastfeeds on demand (whenever the baby shows hunger cues) will usually have a stronger milk supply than one who schedules feeds and misses baby’s cues. On the other hand, if milk is not removed often, production naturally slows down. This cycle ensures the body does not waste energy making more milk than the baby actually needs. It’s the body’s built-in system for efficiency and balance.
Hormonal Regulation: Hormonal regulation refers to the way hormones control important body functions, including milk production and release during breastfeeding. Prolactin and oxytocin are two key hormones in this system, but others—like estrogen and progesterone—also play roles, especially during pregnancy. For instance, during pregnancy, high progesterone prevents full milk production, but after birth, when progesterone drops, prolactin can fully take over to start milk supply. Hormonal regulation makes sure the right processes happen at the right time to support both the parent and baby. For example, when hormones are balanced, the parent can produce enough milk, feel calm during feeding, and recover after birth. This shows how interconnected the whole body is during lactation.
FAQs: Hormonal Regulation of Milk Supply
-
Scenario: A parent notices milk leaking even before picking up their baby.
Answer: This happens because oxytocin is released when you hear your baby cry, see your baby, or even think about them. Oxytocin contracts the milk ducts and pushes milk toward the nipple, even if your baby isn’t latched. It’s a normal reflex called let-down. -
Scenario: A parent worries because they never feel the “pins-and-needles” sensation others describe.
Answer: Not everyone feels the let-down reflex. What matters most is if your baby is swallowing well, gaining weight, and producing plenty of wet diapers. Those are stronger indicators of milk transfer than physical sensations. -
Scenario: A parent is confused after reading about “two hormones” involved in lactation.
Answer: Prolactin stimulates your breasts to make milk. Oxytocin makes the muscles around the milk glands contract, so milk is released (let-down). Both work together—baby’s sucking boosts prolactin for future milk and oxytocin for immediate flow. -
Scenario: Back at work, the pump yields little the first 5 minutes.
Answer: Use your pump’s let-down mode (fast/light suction) for ~1–2 minutes, then switch to expression (slower/stronger). Watch a baby video, smell a worn baby onesie, or do a 60–90 second warm breast massage before pumping. Correct flange size (nipple moves freely, minimal areola pulled) protects oxytocin release and yield. -
Scenario: Milk leaks during intimacy, while showering, or even at work when thinking about baby.
Answer: Yes, that’s normal. Oxytocin release isn’t limited to feeding—it can be triggered by emotions, sounds, or touch. Wearing breast pads or pressing gently on the breasts through clothing can help control leaking in unexpected situations.
Breastfeeding | 3D Animation

3. The Letdown Reflex
Learning Objectives
Define the letdown reflex and describe how it works.
Identify common sensations and cues associated with letdown.
Recognize normal variations and challenges in letdown reflex.
Definition & Explanation
The letdown reflex—also called the milk ejection reflex—is the process where milk is released from the breast in response to oxytocin. When a baby suckles at the breast, oxytocin causes the muscles around the alveoli to contract, pushing milk through the ducts and out the nipple.
Parents often describe letdown as a tingling, warmth, or tightening in the breast, but not everyone feels it. Some may notice milk leaking from the other breast or dripping without nursing. The letdown reflex can also be triggered by emotional or sensory cues, such as hearing a baby cry or thinking about the baby.
Example: Think of letdown like turning on a faucet. The water (milk) is already there, but oxytocin turns the handle so the milk flows.
Scenarios & Tips
Scenario: A parent says, “I leak milk when I hear another baby cry—is that normal?”
Response: “Yes, that’s your body responding to a cue. Your brain releases oxytocin, which triggers letdown.”
Tip: Normalize these experiences to reduce parent worry.Scenario: A parent says, “I don’t feel any tingling—does that mean I’m not having letdown?”
Response: “Not everyone feels letdown. If your baby is swallowing and gaining weight, your letdown is happening even if you don’t feel it.”
Tip: Focus on baby’s feeding cues instead of sensations.Scenario: A parent says, “My milk sprays out really forcefully and my baby coughs.”
Response: “That’s called overactive letdown. It can be managed by nursing in a laid-back position or letting the initial spray flow into a cloth before latching.”
Tip: Offer practical positioning advice to ease feeding.
Evidence-Based Insights
In the study “Comparison of maternal milk ejection characteristics during pumping using infant-derived and 2-phase vacuum patterns” (Gardner, Kent, Lai, Geddes, & Hartmann, 2019), researchers tested whether using a breast pump pattern that more closely mimics infant sucking (versus a standard 2-phase pumping pattern) would change the number or characteristics of milk ejections (i.e. letdowns) or milk removed. They recruited lactating mothers at various stages and measured, during pumping, how many ejections occurred, peak milk flow, and percent of available milk removed. They found no significant difference between the infant-derived pattern and standard pattern in the number or timing of milk ejections or in how much milk was removed. This suggests that the basic physiology of letdown is relatively robust—i.e. the pattern of hormone-driven ejections is not easily altered by small changes in external stimulus. Thus, while multiple letdowns do occur, they seem to follow an individual “preset” pattern that is fairly stable across different stimulation modalities. (Gardner et al., 2019) BioMed Central
In another classic (but still highly relevant) study, “Milk ejection patterns: an intra-individual comparison of breastfeeding and pumping” (Gardner, Ramsay, Hartmann et al., 2015), researchers used ultrasound and milk flow measurement to compare how milk ejection (letdowns) behaves when an infant breastfeeds versus when a mother uses a breast pump. They found that within individual mothers, the number, timing, and duration of milk ejections were quite consistent regardless of whether the breast was stimulated by a baby or by a pump. That is, a mother’s pattern of letdowns tends to be stable across modes of milk removal. (Gardner et al., 2015) PMC
Suggestions for lactation specialists
Recognize that multiple letdowns across a feed are normal, but the specific “schedule” of letdowns (how many, how spaced) is relatively stable per individual, and not easily changed by external tools or techniques.
When supporting pump users, acknowledge that optimizing flange fit, vacuum, and comfort is important—but also know that you may not be able to “force” additional letdowns beyond what the mother’s physiology naturally yields.
Emphasize consistency in feeding or pumping frequency: because letdown patterns are stable, ensuring regular removal is key to sustaining milk flow.
When teaching parents about letdown cues, frame them not as rigid signals but as helpful feedback—encourage observation of baby’s sucking/swallowing changes and reassure that absence of strong cues doesn’t always indicate a problem.
If a parent reports weak or delayed letdown, assess for impediments (stress, discomfort, nipple sensitivity) rather than assuming their physiology is wrong. Use supportive strategies to reduce inhibition (relaxation, comfortable environment) rather than trying to override physiology.
Key Terms & Definitions
Letdown Reflex: The letdown reflex is the natural process where oxytocin, a hormone released in the brain, signals the milk ducts to release milk. This reflex often happens when a baby latches and begins sucking, but it can also occur when a parent hears their baby cry or even thinks about their baby. Some parents describe a tingling or warm sensation in the breasts as milk begins to flow. For example, a mother might feel letdown start while watching a video of her baby. Understanding this reflex helps explain why milk sometimes leaks unexpectedly, especially in the early months of breastfeeding. It is the body’s way of ensuring milk is available whenever the baby needs it.
Milk Ejection: Milk ejection refers to the physical contraction of the small sacs in the breast, called alveoli, that push milk into the ducts so it can reach the nipple. This contraction is triggered by the letdown reflex and makes milk accessible to the baby. Without milk ejection, milk would remain stored in the alveoli instead of being delivered to the infant. For instance, when a baby sucks rhythmically, these contractions occur in waves to provide steady milk flow. Some mothers notice milk spraying when their baby unlatches suddenly, which is a clear sign of milk ejection. It is an essential step for efficient feeding and milk transfer.
Overactive Letdown: Overactive letdown happens when milk flows too forcefully, making it difficult for babies to coordinate sucking, swallowing, and breathing. Babies may choke, cough, or pull away from the breast during feeds. Parents sometimes notice milk spraying strongly if their baby unlatches, which can feel overwhelming to the infant. For example, a baby with an overactive letdown might gulp quickly and become gassy afterward. While this can be stressful, techniques like nursing in a laid-back position or expressing a little milk before latching can help. Recognizing overactive letdown helps parents and lactation consultants adjust feeding strategies to keep both baby and parent more comfortable.
Cues: Cues are signals that trigger the letdown reflex, preparing the body to release milk. These can be physical, such as nipple stimulation, or emotional, like hearing a baby cry or even thinking about feeding. Some parents experience letdown when they smell their baby’s blanket or hear another infant crying. These triggers show how closely the brain and body are connected during lactation. For example, pumping milk may be easier if a parent looks at photos or videos of their baby. Recognizing and using cues can make milk expression more efficient and feeding sessions smoother.
FAQs about the Let-Down Reflex (Milk Ejection Reflex)
-
Scenario: 3-day postpartum parent who never feels tingles or pins-and-needles.
Answer: Many people never feel let-down, and that’s normal. Look instead for signs: baby’s sucking changes from quick “flutter” sucks to slow, deep swallows; you hear rhythmic gulping; milk appears in the pump; or the other breast leaks. If baby has 6+ wet diapers after day 5, steady weight gain, and softening breasts after feeds, your let-down is happening. -
Scenario: 2-week-old sputters at the start of feeds; parent feels a strong spray.
Answer: That’s often a fast let-down. Try laid-back (reclined) nursing so gravity slows flow, or start with hand-expressing/pumping 1–2 minutes before latching. Offer one breast per feed (“block feeding” only with guidance), burp after the initial fast flow, and let baby pause as needed. Most babies adapt within weeks. -
Scenario: At a noisy family gathering, it takes 5–8 minutes for milk to flow.
Answer: Stress hormones can blunt oxytocin release. Build a short pre-feed routine: deep belly breaths (4 in/6 out for 2 minutes), shoulder rolls, warmth on the breast, a sip of water, and looking at baby photos/video. A quiet corner or noise-canceling headphones can help. Consistency usually shortens time-to-let-down. -
Scenario: Back at work, the pump yields little the first 5 minutes.
Answer: Use your pump’s let-down mode (fast/light suction) for ~1–2 minutes, then switch to expression (slower/stronger). Watch a baby video, smell a worn baby onesie, or do a 60–90 second warm breast massage before pumping. Correct flange size (nipple moves freely, minimal areola pulled) protects oxytocin release and yield. -
Scenario: Around 3 months, tingling fades and breasts feel softer.
Answer: Supply and let-down often feel subtler as your body regulates. Softer breasts aren’t low supply if diapers/weight are normal. Babies also get more efficient. If diapers drop, feeds shorten drastically with fewer swallows, or weight gain slows, get a weight check and a latch/pump assessment.
All About Breastmilk Letdowns | What is the milk ejection reflex?
Module 1: Foundations of Human Lactation
Lesson 1.1 Quiz: The Anatomy & Physiology of Lactation
Test your understanding of breast structure and function, the hormones that regulate milk production, and how the letdown reflex works. Several questions present real client conversations — apply the science in plain, accessible language.
1. Which structures in the breast are responsible for producing milk?
✓ Correct! Alveoli are the tiny, grape-like clusters where milk is actually synthesized. The ducts then transport that milk toward the nipple.
✗ Not quite. The alveoli produce milk, while the ducts transport it. The areola surrounds the nipple, and fatty tissue gives the breast its shape but doesn't produce milk.
2. Which hormone is primarily responsible for milk synthesis?
✓ Correct! Prolactin signals the alveoli to produce milk. Levels rise with frequent, effective milk removal — which is why supply often follows demand.
✗ Not quite. Prolactin makes the milk. Oxytocin releases it. Estrogen and insulin play supporting roles, but prolactin is the primary milk-synthesis hormone.
3. Which hormone is responsible for triggering milk ejection (letdown)?
✓ Correct! Oxytocin causes the muscle cells around the alveoli to contract, pushing milk through the ducts toward the nipple. This is the letdown reflex.
✗ Not quite. Oxytocin drives letdown. Prolactin produces milk, while cortisol and progesterone don't directly trigger milk release.
4. Scenario: Explaining Supply & Demand
Case Study
A new mother asks, "Why do people keep telling me my body will make more milk if my baby nurses more often?" What's the most accurate plain-language explanation?
✓ Correct! That's the core principle: supply follows demand. Frequent, effective milk removal raises prolactin levels and signals the body to keep producing milk.
✗ Not quite. The principle is supply and demand: more frequent, effective milk removal signals the body to produce more milk. Supply isn't fixed at birth.
5. Scenario: A Mother Concerned About Letdown
Case Study
A mother says, "I'm so stressed that my milk doesn't come down as easily anymore." What's the most science-based response a lactation specialist might offer?
✓ Correct! Oxytocin is sensitive to stress. A calm environment, skin-to-skin contact, deep breathing, and feeling supported all help the letdown reflex work smoothly.
✗ Not quite. Stress absolutely affects letdown by suppressing oxytocin. The supportive answer addresses relaxation and comfort — not medication or stopping breastfeeding.
6. What is the function of the milk ducts?
✓ Correct! Ducts are the transport pathways. They carry milk from the alveoli (where it's made) toward the nipple, where the baby can access it during a feed.
✗ Not quite. Milk ducts transport milk. The alveoli produce it, hormones come from glands like the pituitary, and connective/fatty tissue provides structure.
7. Scenario: A Question About Pumping
Case Study
A returning client asks, "If I pump regularly while away from my baby, will my body keep making milk?" What's the most accurate response?
✓ Correct! What matters is consistent, effective milk removal — through nursing, pumping, or both. The body responds to demand, not the source of removal.
✗ Not quite. Pumping can absolutely maintain supply. The body responds to the signal of milk removal, whether that's from a baby or a pump.
8. True or False: The letdown reflex can be triggered not just by the baby latching, but also by the sound of a baby crying or even thinking about the baby.
✓ Correct! Letdown can be conditioned by sensory and emotional cues — a crying baby, a photo, even thinking about the baby — because oxytocin responds to these triggers.
✗ Actually, true. Letdown can be triggered by sensory cues like sound, sight, or thought of the baby — not just direct latching.
9. Scenario: Educating About the First Days
Case Study
An expectant client asks why frequent feeding in the first days after birth is so important. What's the most accurate physiological explanation?
✓ Correct! Early, frequent milk removal helps establish strong long-term supply by stimulating hormone receptors and the milk-producing cells. The first days set the stage for sustainable lactation.
✗ Not quite. The early days are foundational. Frequent milk removal during this window helps establish — not reduce — long-term milk production.
10. Which statement best summarizes the anatomy and physiology of lactation?
✓ Correct! That's the heart of lactation physiology — anatomy, hormones, and behavior working together as a responsive, dynamic system. Understanding this lets you give clients clear, science-based support.
✗ Not quite. Lactation isn't fixed, isn't driven by one hormone, and isn't identical for everyone. It's a dynamic system involving structure, hormones, and behavior all working together.
-
Breast structure & function. Think of the breast as a small factory with pipes. Milk-making sacs (tiny clusters) produce milk, and small tubes carry it to the nipple. Tiny squeezing cells push milk along. A deep, comfortable latch—baby’s chin pressed to the breast, wide open mouth, rounded cheeks—lets milk flow well and prevents sore nipples.
Hormonal regulation. In late pregnancy the breast makes small amounts of colostrum. After the placenta is delivered, milk volume rises around days 2–4. Two main messengers run the show: prolactin tells the body to make milk, and oxytocin helps release milk. From then on, supply follows use: milk that is removed often (8–12 times in 24 hours) tells the body to make more; milk that sits in the breast tells it to slow down.
Let-down (milk ejection) reflex. When the nipple is stimulated, a signal goes to the brain and oxytocin is released, causing waves of milk to let down. Some parents feel tingling or a sudden rush; it can happen several times in one feed. Let-down is helped by skin-to-skin, warmth, gentle breast massage, and relaxed breathing, and it can be blocked by pain, stress, nicotine, tight clothing, or some medicines—so reduce those barriers first.
-
Geddes, D. T., & Sakalidis, V. S. (2016). Sucking dynamics of breastfeeding infants. Seminars in Fetal and Neonatal Medicine, 21(3), 134–139. https://www.sciencedirect.com/science/article/pii/S1744165X16300217
Kent, J. C., Gardner, H., & Geddes, D. T. (2016). Breastmilk production in the first 4 weeks after birth of term infants. Nutrients, 8(12), 756. https://www.mdpi.com/2072-6643/8/12/756
Neville, M. C., & Morton, J. (2001). Physiology and endocrine changes underlying human lactogenesis and milk secretion. The Journal of Nutrition, 131(11), 3005S–3008S. https://academic.oup.com/jn/article/131/11/3005S/4686950
Ramsay, D. T., Kent, J. C., Hartmann, R. A., & Hartmann, P. E. (2005). Anatomy of the lactating human breast redefined with ultrasound imaging. Journal of Anatomy, 206(6), 525–534. https://onlinelibrary.wiley.com/doi/10.1111/j.1469-7580.2005.00426.x
Uvnäs-Moberg, K., Prime, D. K., & Geddes, D. T. (2019). Oxytocin effects in mothers and infants during breastfeeding. Acta Paediatrica, 108(6), 1033–1044. https://onlinelibrary.wiley.com/doi/10.1111/apa.14745
Victora, C. G., Bahl, R., Barros, A. J. D., França, G. V. A., Horton, S., Krasevec, J., … Rollins, N. C. (2016). Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. The Lancet, 387(10017), 475–490. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(15)01024-7/fulltext
World Health Organization. (2009). Infant and young child feeding: Model chapter for textbooks for medical students and allied health professionals (WHO/UNICEF). https://apps.who.int/iris/handle/10665/44117
Academy of Breastfeeding Medicine. (2018). ABM Clinical Protocol #9: Use of galactogogues in initiating or augmenting maternal milk production, with cautionary note (Revised)—PDF. https://abm.memberclicks.net/assets/DOCUMENTS/PROTOCOLS/9-galactogogues-protocol-english.pdf
Academy of Breastfeeding Medicine. (2020). ABM Clinical Protocol #32: Hyperlactation—Diagnosis, management, and prevention—PDF. https://abm.memberclicks.net/assets/DOCUMENTS/PROTOCOLS/32-hyperlactation-protocol-english.pdf
Wambach, K., & Spencer, B. (2021). Breastfeeding and human lactation (6th ed.). Jones & Bartlett Learning. https://www.jblearning.com/catalog/productdetails/9781284223127
Lawrence, R. A., & Lawrence, R. M. (2021). Breastfeeding: A guide for the medical profession (9th ed.). Elsevier. https://www.elsevier.com/books/breastfeeding/9780323680137